Download
1 / 15
180 likes | 355 Views
Statin Induce Myotoxicity. นสภ.อัจจิมา บัวหลวงงาม. Risk of myotoxicity. all statins can cause myopathy with a risk of progressing to rhabdomyolysis . The risk appears to increase with higher doses. Lipophilicity >>> hydrophillic lipophilic

E N D
Statin Induce Myotoxicity นสภ.อัจจิมา บัวหลวงงาม
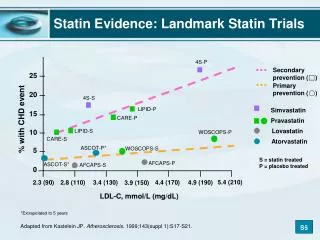
Risk of myotoxicity • all statins can cause myopathy with a risk of progressing to rhabdomyolysis. • The risk appears to increase with higher doses. • Lipophilicity>>>hydrophillic • lipophilic • Atorvastatin, Fluvastatin, Lovastatin, Simvastatin • hydrophilic • Pravastatin, Rosuvastatin
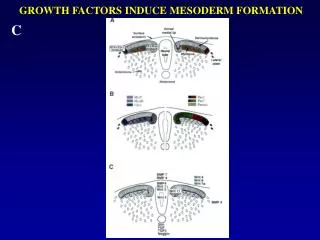
Mechanism HMG-CoA HMG-CoAreductase Statins mevalonate antioxidant and membrane stabilizer that is utilized by mitochondria for electron transport Atrogin-1 ubiquinone (coenzyme Q10) mitochondrial adenosine triphosphate (ATP)
Classification of Muscular Adverse Events Br J Cardiol,2005
Classification of Muscular Adverse Events Br J Cardiol,2005
The American College of Cardiology/American Heart Association/National Heart, Lung, and Blood Institute (ACC/AHA/NHLBI) • 1. Statin myopathy: muscle complaints related to statin drug use • 2. Myalgia: muscle complaints without serum CK elevations • 3. Myositis: muscle symptoms with serum CK elevations • 4. Rhabdomyolysis: markedly elevated CK levels, usually > 10 times ULN, with an elevated creatinine level consistent with pigmentinduced nephropathy J Am Coll Cardiol. 2002; 40: 567-72
สารราชวิทยาลัยอายุรแพทย์ฯสารราชวิทยาลัยอายุรแพทย์ฯ • myopathy • มีอาการกล้ามเนื้ออักเสบร่วมกับระดับของ creatine kinase (CK)>10 เท่า ของ ULN สารราชวิทยาลัยอายุรแพทย์ฯ ปีที่23 ฉบับที่ 3 กรกฎาคม–ธันวาคม 2549
The National Lipid Association • rhabdomyolysis • muscle cell destruction or enzyme leakage, regardless of the CK level when measured, • considered to be causally related to a change in renal function (Thompson et al 2006).
The National Lipid Association • Classify absolute CK elevation • Mild: CK increases < 10 times ULN • Moderate: CK increases ≥ 10 times ULN, and • Severe: CK increases ≥ 50 times the ULN (Thompson et al 2006).
Time to onset • Mean duration of thereapy • 6.3 months (0.25-48 months)
Incidence • Myalgia without changes in CK levels (Bays 2006). • 21 statin-based clinical trials with over 180,000 person years for evidence of muscle toxicity. • The incidence of myopathy was 11 per 100,000 person-years. • The incidence of rhabdomyolysis in 2 cohort studies was 3.4 (1.6–6.5) per 100,000 person-years • 10-fold higher when gemfibrozil was used in combination with statins. • For statins metabolized by CYP3A4 such as lovastatin, atorvastatin, and simvastatin), the incidence was 4.2 per 100,000 person-years. In this group, interaction with drugs known to inhibit CYP3A4 (ie, erythromycin and azoleantifungals) occurred in 60%
The American Journal of Cardiology. Vol 97 (8A) April 17, 2006
The American Journal of Cardiology. Vol 97 (8A) April 17, 2006
Monitor transaminase level • When start Statin or fibrates • After medication 6-12 weeks • Follow up every 1-2 time per year • High dose or more than 2 medication • 3-6 months Guidelines for Management of Dyslipidemia,สารราชวิทยาลัยอายุรแพทย์ฯ 2545