Download
1 / 39
540 likes | 1.37k Views
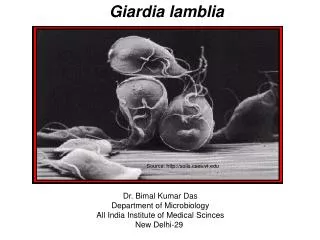
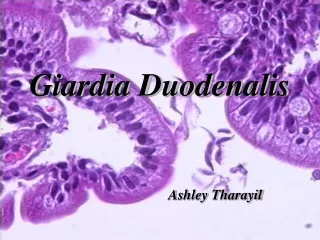
Giardia Lamblia. introduction. It has a worldwide distribution and is the most common pathogenic protozoan isolated from human stools. Symptomatic giardiasis is characterized by acute or chronic diarrhea and/or other gastro-intestinal manifestations. (tourer’s diarrhea).

E N D
introduction • It has a worldwide distribution and is the most common pathogenic protozoan isolated from human stools. • Symptomatic giardiasis is characterized by acute or chronic diarrhea and/or other gastro-intestinal manifestations. (tourer’s diarrhea) • 200 million cases per year.
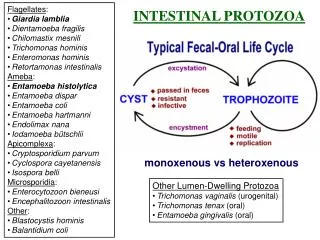
Morphology 1. Trophozoite Typically 12-15 μm in length, 5-10 μm wide, and 2-4 μm thick. Nuclei (Nu): two Karyosomes (k): larger Median bodies (MB): two Adhesive disk (AD): one Axonemes (Ax): a pair Flagella (Fg): 4 pairs --anterior, posterior-lateral, caudal, ventral
Morphology 2. cyst The cysts are oval shaped and typical measure 11-14 μm in length and 6-10 μm wide. Nuclei (Nu): four Karyosomes (k): larger Axonemes (Ax): Median bodies (MB): Cyst wall (CW):
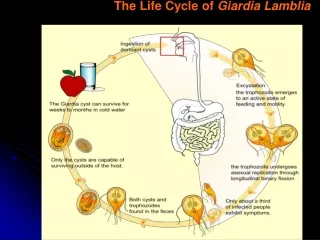
Life cycle in colon ingested, excystation in the small intestine trophozoite trophozoite Mature cyst Cyst Be passed in formed stood Binary fission Located the duodenum and jejunum
pathogenesis • obstruct absorption : 2. produce a mechanical irritation : 3. lead to lactase deficiency as well as other enzyme deficiencies in the microvilli: Covering of the intestinal epithelium by the trophozoite and flattening of the mucosal surface results in malabsorption of nutrients, osmotic diarrhea.
pathogenesis • obstruct absorption : 2. produce a mechanical irritation : Shortening of the villi, crypt cell hypertrophy, and increased inflammatory cell infiltration in local site.
pathogenesis • obstruct absorption : 2. produce a mechanical irritation : 3. lead to lactase deficiency as well as other enzyme deficiencies in the microvilli: Present mushy stools and excessive gas following treatment
Frequency of various symptoms in persons infected with G.lamblia
Diagnosis . Stool examination . Examining duodenal fluid for trophozoites . Duodenal aspirate or biopsy . Immunological diagnosis ① Formed stools A direct smear stained by Iodine/Iron hematoxylin for cyst.
Cysts of Giardia lamblia,stained with iron- hematoxylin (A, B) and in a wet mount (C; from a patient seen in Haiti). Size: 8-12 µm in length. These cysts have two nuclei each (more mature ones will have four). Giardia lamblia cyst.
Giardia lamblia cyst. Iodine stain. CDCDPDx Parasite Image Library
Giardia lamblia cyst. Iodine stain. CDCDPDx Parasite Image Library
Diagnosis . Stool examination ① Formed stools A direct smear stained by Iodine/Iron hematoxylin for cyst. ② diarrheic stools A direct saline smear for motile trophozoites. 1) fresh stools 2) in time 3) keep warm in cold weather
Diagnosis . Stool examination . Examining duodenal fluid for trophozoites • Intubation. • string test.
Diagnosis . Stool examination . Examining duodenal fluid for trophozoites . Duodenal aspirate or biopsy . Immunological diagnosis
Giardia lamblia. Indirect fluorescent antibody stain. Negative test. Giardia lamblia. Indirect fluorescent antibody stain. Positive test. Giardia - Fluorescent Antibody (FA) StainingPhoto Credit: H.D.A. Lindquist, U.S. EPA
Diagnosis . Stool examination . Examining duodenal fluid for trophozoites . Duodenal aspirate or biopsy . Immunological diagnosis
Epidemiology Distribution: Worldwide The incidenceis estimated at 200 million cases per year.
Epidemiology(refer to that of E.h.) • Epidemic factors • Source of infection : asymptomatic carrier or only mildly afflicted patients. • The cysts are relatively resistant to bad condition of environment. • Disposal of human feces is inadequate, and lead to contamination of food or water with fecal material. • The housefly and the cockroach is animportance factor in the transmission of the disease.
Treatment and control 1.Infected individuals treatment : Metronidazole (cure rates approximately 85% ) Other effective drugs include: quinacrine, tinidazole, furazolidone, and paramomycin. 2. Sanitary disposal of feces . 3. Protecting water supplies from contamination. 4. Health education in regard to improving personal hygiene, drinking boiled water, hand washing 5. Killing the housefly and the cockroach.
introduction • Trichomoniasis is a common sexually transmitted disease with a worldwide distribution. • to cause acute or chronic vaginitis, acute or chronic urethritis and prostatitis. • 2-3 million new symptomatic infections per year in the United States.
Morphology axostyle (ax) : to protrude from the posterior end flagella (fg) : 5 undulating membrane (um): The combined basal bodies (bb): the costa (cs): the cytostomal groove (cy) : A single nucleus (nu): at the anterior end
Life cycle Trichomonas vaginalis resides in the vagina, urethra and prostate , where it replicates by binary fission . Trichomonas vaginalis is transmitted among humans, its only known host, primarily by sexual intercourse (direct contact), Non-venereal transmission ( indirect contact ) is rare. Infective stage: trophozoit.
glycogen acid PH Lactic acid-producing bacteria Pathogenesis 1. The organism causes contact-dependent damage to the epithelium of the infected organ. 2. Associated with a lowered acidity of the vagina, along with a thinner epithelium and less glycogen in the cells. Mechanism of vaginitis caused by T. vaginalis 3.5 to 4.5 utility disrupt acid PH T. vaginalis pH > 5.9
Symptoms Women: 1. Asymptomatic (15%): 2. acute or chronic vaginitis: 3. acute or chronic urethritis: .a copious, foul-smelling discharge that is often gray, frothy or blood tinged ,but can be yellow or green . .burning in vagina or itching on labium ,
Symptoms Women: 1. Asymptomatic: 2. acute or chronic vaginitis: 3. acute or chronic urethritis: . disuria (painful urination) and frequent urination..
Symptoms Men: • Asymptomatic (50-90% ) : • tends to be self-limiting. • 2. acute or chronic urethritis and prostatitiss: • urethral discharge (ranging from scant to prululent), disuria, and urethral pruritus (itching).
Diagnosis Clinical suspicion may be confirmed by finding the trophozoites in vaginal, urethral, prostatic secretions, or urine sediment (following prostate massage). . A direct saline smear for motile trophozoites. . Giemsa-stained smears.
Treatmentand Control 1. Trichomoniasis treatment 1) Drug: Metronidazole, Tinidazole 2) Restore the acidity of the vagina, douching vagina with 1:5000 potassium permanganate solutions. ★ Sexual partners should be treated at the same time to prevent reinfection 2. limiting number of sexual partners and use of condoms . 3. sterilizing of the contaminated toilet articles; detection of infected males should be helpful in reducing infections.
Summary1 • Giardia lamblia • Trichomonas vaginalis
Summary1 • Giardia lamblia Infective stage: mature cyst. • Trichomonas vaginalis Infective stage: trophozoit.
Summary2 • Giardia lamblia Infection occurs by the ingestion of cysts in contaminated water, food, or by the fecal-oral route (hands or fomites). • Trichomonas vaginalis to be transmitted among humans, primarily by sexual intercourse (direct contact), Non-venereal transmission ( indirect contact ) is rare.
Summary3 • Giardia lamblia resides in the duodenum and jejunum • Trichomonas vaginalis resides in the vagina, urethra and prostate
Summary4 • Giardia lamblia often watery, diarrhea. The stool contains excessive lipids but very rarely any blood or necrotic tissue. • Trichomonas vaginalis acute or chronic vaginitis, acute or chronic urethritis and prostatitiss.
Summary5 • Giardia lamblia Metronidazole • Trichomonas vaginalis Metronidazole