Download
1 / 34
350 likes | 589 Views
CPOE Implementation in the Community Setting. What do you need to know? Avoid a Towering Inferno by creating a burning platform Avoid medical staff revolution with the evolution of a patient safety culture. Scope of the Challenge.

E N D
CPOE Implementation in the Community Setting What do you need to know? • Avoid a Towering Inferno by creating a burning platform • Avoid medical staff revolution with the evolution of a patient safety culture
Scope of the Challenge Current and Projected CPOE Implementation at U.S.A. Hospitals 100% 90% 80% 70% 60% US-2005 50% US-2010 40% 30% 20% 10% 0% <300 beds >300 beds US estimates from Kaushal R, et al. Health Affairs 2005;24:1281-1289.
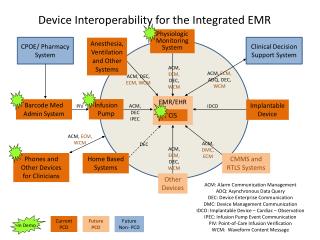
CPOE is a key component of any medication safety initiative PO Medication Delivery CPOE Provider writes order PO med Smart IV Pump IV med Decision Support Pharmacy Pharmacist Approves Order Completing The Loop: Web Reporting Team Training Medication Reconciliation Improving Transitions Electronic Identification Pump sends documentation To eMAR; RN verifies ADE Surveillance eMAR RN acknowledges Approved order Delivery to Site Med Repackaging omnicell, robotics, etc.
CPOE Implementation in the Community Setting Factors Critical for Success • Communicate Vision, Rationale and Goals • Provide Data to Support Vision, Reinforce Benefits and Measure Performance • Demonstrate Leadership Commitment • Mentor Physician Champions • Develop Incentives and Sanctions • Respond to Physician Concerns • Marketing and Communication
Communicate, Communicate, Communicate Vision, Rationale and Goals • CPOE has been proven to enhance patient care. • CPOE reduces medication errors and provides alerts for potential drug interactions and when dosage adjustments are required. • Define firm targets: “75% of medication orders entered electronically by June 2007”
Data to Support Vision and Rationale Serious Medication Error Rates Before and After CPOE 12 10 Phase I (Before CPOE) 8 Serious Medication Errors (Events/1,000 Patient Days) Phase II (After CPOE) 6 4 Delta = -55% P < .01 2 0 Bates et al.: “Effect of Computerized Physician Order Entry and a Team Intervention on Prevention of Serious Medication Errors,” JAMA 1998.
CPOE provides real advantages in providing quality patient care • Quality and safety benefits from decision support tools • CPOE continuously delivers evidence-based treatment. • Care is more reliable, more efficient, and safer • All involved physicians know patient’s medications • Fewer call backs from pharmacy • Fewer call backs from nursing • Faster delivery of inpatient medications • Physician orders are legible
5.0 4.5 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 Data to Reinforce CPOE BenefitsMedication Errors Before and After CPOE Implementation NSMC Adult Psychiatry CPOE live on 9-9-05 NSMC Geriatric Psychiatry CPOE live on 11-8-05 0.3 4.6 Errors Per Month Jan. ’05 – March ‘06 0.4 2.3 0.1 1.7 Actual 0.1 Potential BEFORE AFTER BEFORE AFTER
Why we need to adopt CPOE now? • It is widely accepted as the new standard of care. • It distinguishes our quality of care from hospitals that are late adopters. • It is increasingly a significant point of leverage in negotiations to maximize reimbursement from private insurers.
Demonstrate Leadership Commitment • Hospital Executives and Physician Leaders play formal roles. • NSMC Chiefs Forum reviews CPOE progress every 2-4 weeks. • CEO and President participates in discussion once per month; ad hoc meetings as needed. • Appointment of IS medical director; CMIO • Create the necessary infrastructure to effect change.
Medical Staff LeadershipReporting and Accountability Structure
Leadership and Governance • Chiefs Forum (CF) assumed responsibility as the CPOE Physician Advisory Group. • CF develops policy recommendations, identifies areas of resistance, reviews physician utilization and provides communication. • Medical Executive Committee functions as the governing body of the medical staff. • Education and engagement of Board of Trustees on a regular basis
Expect mixed reaction and pushback during initial rollout • Big Bang vs Sequential Implementation - Initial focus on medication orders at NSMC • MD compliance variable • MDs will complain about the length of time it takes to enter orders compared to writing on paper. • Large practices without hospitalists place a significant burden on rounding MDs
Moving the Ball Forward Focus on steady progress • 24/7 “at the elbow” technical support • Usability enhancements will help with overall acceptance -Process to prioritize order set development -System speed and responsiveness • Identify and mentor high volume, high compliance CPOE users as physician champions.
Monitoring and Reporting • Data for orders entered via CPOE are very accurate • Accurately identifying the ordering MD on paper orders is required for accurate CPOE compliance reports - Encourage second identifier on written orders i.e. print name, beeper #, etc - Orders with illegible signatures are attributed to the attending MD • Weekly reporting to Department Chairs - Numerator: Medication Orders Entered Into CPOM by prescriber - Denominator: Total Medication Orders by prescriber
Weekly Utilization Metrics *Full names provided on actual report.
Pharmacy Study of Handwritten OrdersMay 22, 2006 – June 2, 2006 Accurately identifying the Ordering MD on paper can be a challenge due to illegible signatures
Achieving a “Tipping Point” through Physician Level Reporting • Chairs need to focus on high volume/low compliance MDs. • For those who continue to write on paper, a tougher compliance policy is needed.
Incentives and Sanctions • CPOE P4P incentives ideally aligned with physicians and hospitals. • Consider recognition, contests and give-aways. • Mandatory Training -All physicians must attend a CPOE education class prior to receiving system login. -New medical staff receive training as part of the orientation process.
Sanctions required for those who continue to write on paper NSMC CPOE Compliance Policy & Process • Individual CPOE compliance set at 85%. • Department Chairs own primary management responsibility • MDs have multiple opportunities to remediate their compliance. • Compliance policy patterned after Medical Records completion policy. • Written notification of deficiency, with cc: to chief/chair. • Appearance before Medical Executive Committee. • Suspension of privileges.
Letter describing CPOE compliance policy sent to entire medical staff CPOE Utilization Compliance Policy
Pay for Performance Quality Measures Family Balance Respond to Physicians’ Concerns Demands on Massachusetts Physicians Continue to Increase Declining Reimbursements Increasing Practice Expenses Malpractice Premiums High Cost Of Living Transparency/ Public Reporting CPOE / EMR
Nursing Unit Implications • Routine Verbal Orders are not allowed per JCAHO standards • Telephone Orders will only be accepted for urgent orders or when CPOE is not accessible. • CPOE support staff and RN super users will offer to show MDs how to enter orders. If rebuked, Nurse Manager or Supervisor explains hospital policy regarding reporting of the incident to the Department Chair.
Marketing and Communication • Develop a logo • Heighten awareness; reaffirm commitment to CPOE • Weekly on-line and paper newsletter – publish go-live dates, FAQs, tips • Hold regular informational meetings. • Post signage on each unit reminding MD that “this is a CPOE unit”
Non-CPOE Entered by MD into CPOE % CPOE Measuring CPOE Performance Non-CPOE
Non-CPOE Entered by MD into CPOE % CPOE Measuring CPOE Performance
CPOE Implementation in the Community Setting The Final Move • Remove all paper order sets from the floors. • “As of _________, written orders will not be accepted and all routine orders must be entered via CPOE.”
CPOE Implementation in the Community Setting Final Thoughts and Key Take-Aways • Patient Care is safer • Adopting CPOE requires commitment by busy physicians • Appeal to sense of professionalism • Time is required, but time is saved. • Physicians respond to data • Recognize physician champions • Explore physician incentives and sanctions • Increase financial incentives that reward use
CPOE Implementation in the Community Setting Final Thoughts and Key Take Aways • Respond to physician concerns -Continue efforts to improve the ease of use, speed of the applications and surrounding workflow • Create a patient safety culture that embraces evidence based, standardized, coordinated care • Once you reach a “tipping point,” growing intolerance of non-users • Plan to learn along the way