Download
1 / 37
370 likes | 519 Views
Bone Structure & Dev: Readings. Frankel and Nordin, Chapter 2 Frost, H.M. (2000) Muscle, bone, and the Utah paradigm: A 1999 overview. Medicine & Science in Sports & Exercise , 32:5 , pp 911-917.

E N D
Bone Structure & Dev: Readings • Frankel and Nordin, Chapter 2 • Frost, H.M. (2000) Muscle, bone, and the Utah paradigm: A 1999 overview. Medicine & Science in Sports & Exercise, 32:5, pp 911-917. • Turner, C.H. and Robling, A.G. (2003) Designing exercise regimens to increase bone strength. Ex & Sp Sci Rev, 31:1 pp 45-50. • Modlesky, C.M. and Lewis, R.D. (2002) Ex & Sp Sci Rev, 30:4 pp 111-176. • Humphries, B., et al. (2000) Effect of exercise intensity on bone density, strength, and calcium turnover in older women. Medicine & Science in Sports & Exercise, 32:6, pp 1043-1050.
Bone Structure & Dev Outline • Outline • Structure and architecture • Development and growth • Process – continuous remodeling • Factors affecting bone density and strength • Mechanical properties • Osteoporosis
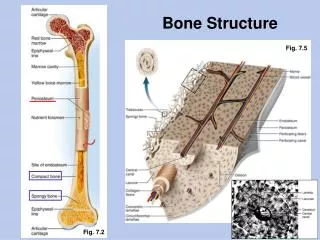
Bone Micro-Structure, cont’d Projections of osteocytes are thought to be cite of strain sensing, which stimulates bone to form
Bone Composition & Structure • Material Constituents: • Calcium carbonate and Calcium phosphate • 60-70% bone weight • Adds stiffness • Primary determinant for compressive strength. • Collagen • Adds flexibility • Contributes to tensile strength • Material Constituents • Water • 25-30% bone weight • Contributes to bone strength • Provides transportation for nutrients and wastes.
Bone Composition & Structure • Structural Organization • Bone mineralization ratio specific to bone • Two categories of porous bone: • Cortical bone(70-95% mineral content) • Trabecular bone (10-70% mineral content) • More porous bones have: • Less calcium phosphate • More calcium carbonate • Greater proportion of non-mineralized tissue
Bone Composition & Structure • Cortical Bone • Low porosity • 5-30% bone volume is non-mineralized tissue • Withstand greater stress but less strain before fracturing
Bone Composition & Structure • Trabecular Bone • High porosity • 30 - >90% bone volume is non-mineralized tissue • Trabeculae filled with marrow and fat • Withstand more strain (but less stress) before fracturing
Bone Composition & Structure • Both cortical and trabecular bone are anisotropic – stress/strain response is directional • Bone function determines structure (Wolff’s law) • Strongest at resisting compressive stress • Weakest at resisting shear stress
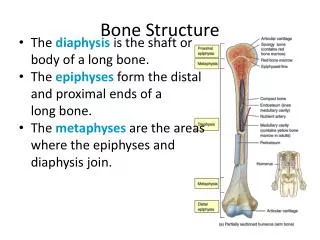
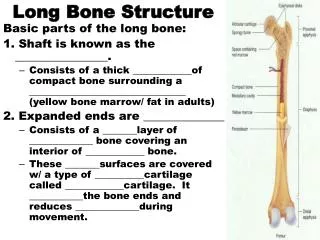
Bone Growth & Development • Longitudinal Growth • at epiphyses or epiphyseal plates • Stops at 18 yrs of age (approx.) • can be seen up to 25 yrs of age • Circumferential Growth • Diameter increases throughout lifespan • Most rapid growth before adulthood • Periosteum build-up in concentric layers • Endosteal growth • Internal remodeling
Bone Growth & Development • Osteoblasts – bone building cells • Osteoclasts – bone absorbing cells • Osteocytes – mature bone cells, embedded in bony matrix in circular pattern • Adult Bone Development • Balance between oseoblast and osetoclast activity • Increase in age yields progressive decrease in collagen and increase in bone brittleness. • Greater in women
Bone Growth & Development • Women • Peak bone mineral content: 25-28 yrs. • 0.5%-1.0% loss per year following age 50 or menopause • 6.5% loss per year post-menopause for first 5-8 years. • Youth – bones are vulnerable during peak growing years • Bone mineral density (BMD) is least during peak growing years • Growth plates are thickest during peak growing years
Bone Growth & Development • Aging • Bone density loss as soon as early 20’s • Decrease in mechanical properties and general toughness of bone • Increasing loss of bone substance • Increasing porosity • Disconnection and disintegration of trabeculae leads to weakness
Bone loading modes: Compression – pushing together Tension – pulling apart Torsion – twisting Shear – cutting across
Stress-strain curve: Load-deformation relationship:
Repetitive vs. Acute Loads • Repetitive loading • Acute loading • Macrotrauma • Microtrauma
I: bone vs glass and metal II: Anisotropic behavior of bone
Comparison of tendon and ligament
Bone Response to Stress • Wolf’s Law • Indicates that bone strength increases and decreases as the functional forces on the bone increase and decrease. • Bone Modeling and Remodeling • Mechanical loading causes strain • Bone Modeling • If Strain > modeling threshold, then bone modeling occurs. • “conservation mode”: no change in bone mass • “disuse mode”: net loss of bone mass • Osteocytes – projections sense strain, or pressure, beginning remodeling process
Bone Response to Stress • Bone mineral density generally parallels body weight • Body weight provides most constant mechanical stress • Determined by stresses that produce strain on skeleton • Think: weight gain or loss and its effect on bone density
Frost’s mechanostat Theory of bone’s Response to stress What factors might Change threshold Levels?
Bone Hypertrophy • An increase in bone mass due to predominance of osteoblast activity. • Seen in response to regular physical activity • Ex: tennis players have muscular and bone hypertrophy in playing arm. • The greater the habitual load, the more mineralization of the bone. • Also relates to amount of impact of activity/sport
Bone Atrophy • A decrease in bone mass resulting form a predominance of osteoclast activity • Accomplished via remodeling • Decreases in: • Bone calcium • Bone weight and strength • Seen in bed-ridden patients, sedentary elderly, and astronauts
Osteoporosis • Website on osteporosis: http://www.nof.org National Osteoporosis Foundation • A disorder involving decreased bone mass and strength with one or more resulting fractures. • Found in elderly • Mostly in postmenopausal and elderly women • Causes more than 1/2 of fractures in women, and 1/3 in men. • Begins as osteopenia
Osteoporosis • Type I Osteoporosis = Post-menopausal Osteoporosis • Affects about 40% of women over 50 • Gender differences • Men reach higher peak bone mass and strength in young adulthood • Type II Osteoporosis = Age-Associated Osteoporosis • Affects most women and men over 70
Osteoporosis • Symptoms: • Painful, deforming and debilitating crush fractures of vertebrae • Usually of lumbar vertebrae from weight bearing activity, which leads to height loss • Estimated 26% of women over 50 suffer from these fractures
Osteoporosis • Men have an increase in vertebral diameter with aging • Reduces compressive stress during weight bearing activities • Structural strength not reduced • Not known why same compensatory changes do not occur in women
Position Statement of ACSM on Osteoporosis • Weightbearing physical activity is essential for developing and maintaining a healthy skeleton • Strength exercises may also be beneficial, particularly for non-weightbearing bones • An increase in physical activity for sedentary women can prevent further inactivity-related bone loss and can even improve bone mass • Exercise is not an adequate substitute for postmenopausal hormone replacement • Ex programs for older women should include activities for improving strength, flexibility, and coordination, to lessen the likelihood of falls
Osteoporosis Treatment • Hormone replacement therapy • Estrogen deficiency damages bone • Increased dietary calcium • Lifestyle factors affect bone mineralization • Risk factors for osteoporosis: • Smoking, alcohol • Inactivity • Low body fat • White, female, postmenopausal
Osteoporosis Treatment • Future use of pharmacologic agents • May stimulate bone formation • Low doses of growth factors to stimulate osteoblast recruitment and promote bone formation. • Best Bet: • Engaging in regular physical activity involving weight bearing and resistive exercise • Avoiding the lifestyle (risk) factors that negatively affect bone mass.
Common Bone Injuries • Stress Fractures • Begin as small disruption in continuity of outer layers of cortical bone. • Occur when there is no time for repair process (osteoblast activity) • Injuries to articular cartilage (osteoarthritis) • Epiphyseal injuries • Injuries to cartilaginous epiphyseal plate • Acute and repetitive loading can cause • Premature closing of epiphyseal junction and termination of bone growth • Osteochondrosis • Disruption of blood supply to epiphyses • Associated with tissue necrosis and potential deformation of the epiphyses. • Injuries to tendon-bone junction, the apophysis • Apophysitis • Osteochondrosis of the apophysis • Associated with traumatic avulsions.