Download
1 / 34
340 likes | 871 Views
Central nervous system. Central nervous system Guanghui Yu Radiology college . Central nervous system. Pituitary adenoma Pituitary adenoma is tumor arising from the cells of the pituitary gland

E N D
Central nervous system Central nervous system Guanghui Yu Radiology college
Central nervous system Pituitary adenoma • Pituitary adenoma is tumor arising from the cells of the pituitary gland • A tumor of less than 10mm in diameter is called a microadenoma and is usually confined within the sella turcica • A macroadenoma is a tumor of more than 10 mm in diameter and usually extends beyond the confines of the sella turcica upward toward the chiasm and hypothalamus downward toward the sphenoid sinus laterally toward the cavernous sinuses
Central nervous system • Pituitary adenomas are usually benign tumors • pituitary carcinomas are very rare • Metastases from pulmonary or breast tumors may grow within the pituitary gland
Central nervous system • prolactinomas and ACTH-secreting tumors are usually microadenomas • GH-secreting adenomas and nonsecreting tumors are usually macroadenomas • Other secreting tumors like TSH-, FSH- or LH-secreting adenomas are very rare ACTH: adrenocorticotrop(h)ic hormone GH: growth hormone TSH: thyrotropic-stimulating hormone FSH: follicle-stimulating hormone LH: luteotrop(h)ic hormone
Central nervous system • Neuroradiological diagnosis is based mainly on MRI findings • The study should be performed with coronal and sagittal thin slice T1-weighted images, without and with contrast enhancement
Central nervous system Pituitary Microadenoma • Neuroradiological diagnosis is nowadays made by MR • CT may also be used but due to the inferior resolution MR is preferred • The CT appearance of a microadenoma is that of an iso- or slightly hypodense nodule of few mm in diameter within the pituitary gland • The microadenoma is better seen after contrast injection since the pituitary tissue enhances(due to the absence of a bloodbrain barrier while the adenoma remains hypodense)
Central nervous system MR • A similar effect is seen with MR; usually only T1-weighted sequences are used and the microadenoma is more evident following gadolinium injection since it appears hypointense within an hyperintense pituitary. Enhancement may be inhomogeneous. • Not infrequently, the nodule is difficult to detect and dynamic techniques may improve the detection rate • Not infrequently the microadenoma may be hyperintense on the baseline T1WI, due to intratumoral bleed
Central nervous system coronal T1WIfollowing gadolinium injection delayed a few minutes A left-sided microadenoma, depressing and eroding focally the sella floor, remains hypointense with respect to the normally enhancing pituitary gland. In the delayed image a focal nodule of enhancement appears within the hypodense component
Central nervous system The patient has Cushing's disease. coronal T1WI following gadolinium injection coronal T1WI without contrast • Mild focal depression of the sellar floor on the right side ; mild focal enlargement and hypointensity of the right half of the pituitary gland. • coronal T1WI following gadolinium injection. The normal pituitary gland enhances homogeneously while the microadenoma remains hypointense.
Central nervous system Pituitary Macroadenoma • A macroadenoma can remain confined within the sella turcica, or it may grow upward, downward, laterally or more commonly in all directions • plain films usually show an expanded sella with erosion and depression of the sellar floor toward the sphenoid sinus • CT shows the same bony changes and the mass lesion, usually isointense, with marked enhancement
MRI better shows involvement of the surrounding structures The tumor is usually isointense on T1-weighted images and shows marked enhancement following gadolinium injection. Sometimes haemorrhagic and cystic components are present
Isointense space-occupying lesion originating from the sella turcica and extending bilaterally, mainly on the right side. The cavernous sinus is invaded on the right side, with encasement of the internal carotid artery . following gadolinium injection of contrast. Marked homogeneous enhancement of the tumor. The superior suprasellar, inferior sphenoidal and lateral cavernous extension of the tumor is well seen. The sella turcica is markedly enlarged, the floor is depressed, the chiasm is compressed and elevated
Acoustic neurinoma • a benign tumor deriving from schwann cells of the acoustic nerve • It is the most frequent intracranial schwannoma • Most commonly the neoplasm originates from the vestibular portion of the eighth cranial nerve • it can be exclusively intracanalicular or may extend as a mass in the cerebellopontine angle
Schwannomas are mainly tumors of adulthood • Histologically, they are encapsulated masses with an ovoid, tubular or lobulated shape • Haemorrhage and necrosis may occur • One quarter of tumors are hypervascular • The earliest symptoms are tinnitus and sensorineural hearing loss
Plain film radiographs can reveal widening of the internal auditory canal. which, however, is a late manifestation of the tumor • On CT axial images intracanalicular schwannomas are usually missed. Larger tumors both intra- and extracanalicular appear as oval or lobulated masses, they may present as a broad base against the petrous ridge at the level of the internal auditory meatus and enlarging the cerebellopontine angle (CPA) cistern . They are iso- to slightly hypodense to brain and show strong but variable enhancement owing to cystic degeneration in larger neoplasms. • Calcifications are rare.
MR images using thin-sections (3mm) will reveal both intra- and extracanalicular schwannomas • round or oval in shape • The signal is slightly hypointense on T1WI and heterogeneously hyperintense on T2WI. The heterogeneous aspect is due to the presence of cysts, areas of different cellular histology, neovascularity and haemorrhage • It should be noted that significant heterogeneity on MRI is more typical of acoustic schwannoma than meningioma • The contrast enhancement of schwannomas is usually marked but frequently inhomogeneous • Contrast medium injection is necessary to detect smaller intracanalicular tumors that may not otherwise be seen
coronal T1WI passing through the internal auditory canals. Arrow point on the barely seen intracanalicular neurinoma. axial T2WI. The lesion is not recognizable within the internal auditory canal on the left side. coronal and axial T1WI following gadolinium injection. Enhancement of the intracanalicular neurinoma (arrow).
Axial CT, bone window. The internal auditory canal on the right is expanded. axial and coronal T1WI following gadolinium injection. Enhancement of the neurinoma, that grows within the cerebellopontine angle cistern, compressing and displacing the brainstem.
Lentiform nucleus Basal ganglia Head of caudate nucleus Genu of Corpus callosum External capsule Internal capsule Thalamus Splenium of Corpus callosum
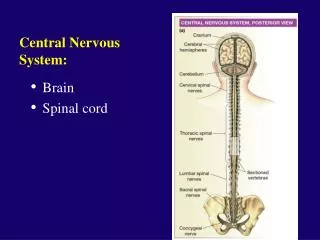
Intracranial Hematoma • Epidural Haematoma • Subdural Haematoma • subarachnoid haemorrhage • intracerebral haematoma • intraventricular haemorrhage Cerebral Infarction
Brain Neoplasm • Astrocytoma • Meningioma • Pituitary adenoma • Acoustic neurinoma
Flowing void effect aneurysm
metastases 4.2a. Post-contrast Axial T1 Wtd MRI 4.2b. Post-contrast Coronal T1 Wtd MRI