Download
1 / 45
960 likes | 3.94k Views
Pharmaceutical solutions. Pharmaceutics (PHM224Y/PHC330Y) Gregory Poon, PhD, BScPhm, RPh. Solution: definition. Homogeneous mixture of two or more substances May exist in any phase Vinegar is acetic acid (and other stuff) in H 2 O Air is a solution of N 2 , O 2 , CO 2 , etc.

E N D
Pharmaceutical solutions Pharmaceutics (PHM224Y/PHC330Y) Gregory Poon, PhD, BScPhm, RPh
Solution: definition • Homogeneous mixture of two or more substances • May exist in any phase • Vinegar is acetic acid (and other stuff) in H2O • Air is a solution of N2, O2, CO2, etc. • Steel is a solution of iron and carbon • We will focus liquid solutions, with H2O or oil as solvent • Solute must be “dissolved” in solvent • Not suspensions
Concentration units • Molarity (M) • mol/L solution • Temperature dependent due to dV/dT (expansivity) • Molality (m) • mol/kg solvent • Not temperature dependent • Mole fraction (X) • Not commonly used pharmaceutically Of k components
More concentration units • Assume 1 g = 1 mL i.e., = 1 • Weight percent • g/100 mL = 10 mg/mL solution (w/v) • g/100 g = 10 mg/g (w/w) • Cream, ointment, gel, etc. • Volume percent • mL/100 mL solution (v/v) • Parts per thousand/million/billion (ppt, ppm, ppb) • ppt = 1 g/1000 mL = 1 g/L • ppm = 1 mg/L • ppb = 1 µg/L • Commonly used to express contamination
Other concentration definitions • H2O2 • Commercial H2O2 expressed as x-volume strengths • 1 vol solution produces 10 vol O2 (at STP) when completely decomposed • 3% w/v solution = 10 vol • Activity units • Vitamin A, D • Enzymes, bioactive proteins • Heparin • Based on arbitrary definition of activity under specified conditions (temperature, pH, etc.) • No correspondence to amount due to (im)purity
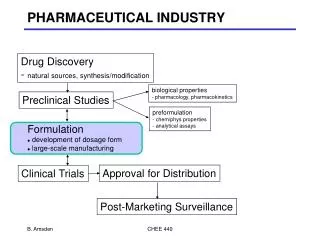
Pharmaceutical solutions: consideration • Route of administration • Oral, IV, IM, SC, nasal, rectal, etc. • Stability of drug solute • Physicochemical • Contamination • Purity • Microbial • Chemical • Containers • Organoleptic factors (oral)
Pharmaceutical solutions: advantages • Easy to dose from concentrate by simple dilution • Easy to mix if necessary • Easy to measure accurately • Volumetric devices can be very precise and accurate if YOU take care • Easy to administer orally to children and disabled persons • Amenable to administration by any route • Ex: suspension cannot be given IV • No lag time due to dissolution • Rapid onset of action
Pharmaceutical solutions: disadvantages • Solution chemistry poses many stability issues • Physicochemical degradation • Shelf life, storage requirement • Reactivity • Containers, tubing, etc. • Shorter expiry than other dosage forms • Additional sterility concerns • Solubility may be limiting • Need to mask taste (oral) • Ex: suspension is “harder” to taste
Aromatic waters + volatile oil Aqueous acids Diluted acids Douches Enemas Rectal or oral Gargles Mouthwashes Irrigation solutions Syrups Concentrated sugar solution Elixir Used to contain EtOH Liniments + organics, oil Spirits Peppermint water, rosewater Acetic acid, HCl(aq) Phosphate enema NS for irrigation Simple syrup (75% sucrose) Aromatic ammonia spirit Solutions: many appellations
Composition of pharmaceutical solutions • Drug • Solvent • Water, possibly with “premade” matrix • D5W, NS, Ringer’s, NaHCO3, etc. • Oil • Cosolvent if needed for solubility • Cosolute • Buffer (for pH) • Additional salts and/or nonelectrolytes • Adjust tonicity • Preservatives • Against microbial contamination • Against chemical degradation • Colour, flavouring agents (oral only)
Pharmaceutical solutions: solvent • “Purified water” (PW) according to USP 23 • Potable water must be further purified for pharmaceuticals • Remove organic and ionic contaminants • Total organic carbon (<500 ppb) • Resistivity (e=RA/l[R m]; >17 M•m at pH 7.0) • Methods • Reverse osmosis (cellulose acetate filters) • Often feed water for further purification • Double distillation (>10 M•m) • Ion exchange resin (>18 M•m) • Product is generally also “sterile”, though not relied on as such (<100 cfu/mL)
Pharmaceutical solutions: oil • Usually IM, sometimes po • Of vegetative origin • Less saturated, lower melting temperature • Keep the vegetarians happy • Ex: peanut, sesame, corn, cottonseed • Becomes rancid when oxidized • Must not contain substances that cannot be metabolized • Mineral oil, paraffin, etc. • Esters of fatty acids give less viscous liquid and easier to inject
Infinite dilution of any acid or base will lead to pH neutrality! Equimolar acetate buffer Buffer capacity and autoionization of water
To make a 50 mM potassium acetate solution … • Dilute 50 mmol acetic acid in ~950 mL water, add concentrated KOH to pH 4.5, and qs to 1 L. • Dissolve 50 mmol potassium acetate in ~950 mL water, titrate pH to 4.5 with concentrated HCl, and qs to 1 L. • Dissolve 50 mmol potassium acetate in ~950 mL water, titrate pH to 4.5 with glacial acetic acid, and qs to 1 L. • Mix 25 mmol acetic acid and 25 mmol potassium acetate to make 1 L of solution. All roads lead to Rome … sort of
Hion van’t Hoff equation Poon et al. (2002) Kozlov and Lohman (2000) Thermodynamics of acid-base equilibria: temperature effects
Conditions that stabilize A-increaseKa Conditions that stabilize HA decreaseKa Conjugate pairs differ by (at least) their net charges, so electrostatic interactions are likely important factors for their relative stabilities. H2O H2O H2O H2O H2O H2O Na+ Na+ Na+ H2O Na+ H2O H2O Na+ A- Na+ H2O H2O Na+ H2O Na+ Na+ H2O H2O H2O H2O H2O H2O H2O H2O H2O Thermodynamics of acid-base equilibria: salt effects
Ions with multiple and/or unshielded charges (high charge density) are highly susceptible to electrostatic interactions Ex: phosphates, borates But not Tris, MES, etc. (Why?) Poon and Macgregor, unpublished Beispiel
This other dude is his buddy J. N. Brønsted Bjerrum length: Charge separation at which coulomb energy equals the thermal energy kT Dielectric constant Thermodynamics of acid-base equilibria: solvent effects
At 25°C… • …in vacuo or in air (D 1), lB = 56.0 nm • …in H2O (D = 79), lB 0.714 nm • So ionic bonds are much weaker in H2O; unpaired charges in nonpolar environment are highly unfavoured
Choosing a buffer salt • What pH? • pKa = pH ± (0.5 to 1) • At what temperature?! At what ionic strength?! • (At what pressure?) • Compatibility with other solutes • Neutral salts • Common ion effect • Phosphates with Ca2+, Mg2+, Zn2+, Mn2+, Cu2+… • Tris with Ag+ • Metal chelation • Tris, tricine, EDTA, EGTA, etc. • Toxicity • Cacodylate, oxalate, etc.
Specific issues • Carbonate • Prone to buffer loss due to dehydration to CO2 • Carbonate buffer <pH 7 will burst into • Buffers with multiple closely-spaced pKa • Citrate, succinate, etc. • Susceptible to pH hopping • Lowest and highest pKa useable as one-way buffer • Not many friendly buffers for pH 5 to 6 • Careful with buffer salts of marginal solubilities • Na vs. K • Titrate pH AFTER you are done with all the solutes, not BEFORE!
Pharmaceutical solutions: cosolvent • Organic liquid used to increase solubility of lipophilic drugs • EtOH, glycerol, PG, PEG, cyclodextrin • For acid or base, increases solubility of unionized drug (S0) • Alters activity of water • Changes pKa • May precipitate ionic cosolutes
Chemical stability of solutions • Main chemical pathways are hydrolysis, oxidation and photochemistry • Hydrolysis • Ex: ASA • Difficult to avoid in aqueous solution • Different mechanisms depending on pH • Keep pH near neutral if feasible • First order in aqueous solution • Zero order in suspension
Oxidation in solution • Dissolved O2 from air • Catalyzed by trace transition metals • Cu, Ni, Fe, Mn, Co, etc. • Contaminants from drug and solutes from which solution was made • Ex: captopril (Lee and Notari, 1987) • Oxidation of oily vehicle (rancid) • Strategies • Purge with inert gas, usually N2 • Antioxidants, EDTA (chelates free metal ions)
Some antioxidants • Electron-rich molecules and happy to share! Butylated hydroxy anisole (BHA) Butylated hydroxy toluene (BHT) Tocopherols Ascorbate Propyl gallate
Photochemical degradation • Absorption of incident photon • Usually UV, but visible photon may be energetic enough • Often results in oxidation of susceptible group • Ex: nifedipine • Mechanistically linked to phototoxicity of some drugs • Keep in light-tight containers
Antimicrobial preservatives • Enemies • Bacteria • Yeast and mold • Alcohol • Ethanol (>10%) • Propylene glycol (15-30%) • Organic acids • Only unionized fraction active (why?) • Examples: • Benzoic acid <0.1% (pKa 4.5) • Sorbic acid <0.1% (pKa 4.8) • Acetic acid (pKa 4.7) • Limited by taste
More antimicrobials • Parabens <0.1% (pKa 8.5) (esters) • Solubility decrease with increasing R • Ester can also hydrolyze • Quaternary ammonium salts <0.02% • Highly water soluble • Acts as surfactant • Not active against Gram-negative bacteria (why?) • Nitrite (cured meat) • Active against C. botulinium • Carcinogenic • Sulfites (wine) • Allergen, flavour problems
Agent pH Range Benzoic acid 2.5-4.0 Sorbic acid 3.0-6.5 Proprionic acid 2.5-5.0 Acetic acid 3.0-5.0 Parabens 3.0-9.0 Sulfites 2.5-5.0 Nitrites 4.0-5.5 Antimicrobials: summary • Defined effective pH ranges • Some also double as antioxidants • Sorbate, sulfites • Oily solutions: surfactants, ex: hexylresorcinol
Endotoxins • Lipopolysaccharide (LPS) complex associated with outer cell membrane of Gram-negative bacteria • Strongly pyrogenic, canlead to septic shock • Very persistent • Harsh removal • 250°C x 45 min. • Strong alkali oroxidizer • Limit for WFI: 0.25 U/mL • Only good strategy is testvigorously and avoidsources
Pharmaceutical solutions: tonicity • Important especially for parenteral solutions • Paratonic solutions can present significant osmotic toxicity • Hypotonic (cells explode) • Hypertonic (cells crenate) • Pain! • Can use hypertonicity as an antimicrobial strategy • Ex: sucrose solution (>60%) is self-preserving • Remember osmotic pressure () is colligative property • Not specific to any particular solute • Implications for strong and weak electrolyte • Ex: NaCl vs. NaAc • pH dependence
Tonicity: more subtle than osmotic pressure • “Iso-osmotic” does NOT imply “isotonic” • Some solutes cannot penetrate certain membranes • Ex: boric acid and mannitol cannot enter RBC • Iso-osmotic solution will be hypertonic if given IV! • Must consider specificity of tissue being exposed • Ex: boric acid okay for ophthalmic and nasal tissues • Paratonic solutions can be intentional • SC injections • Fatty tissue more tolerant • IM injections • Hypertonic formulation to draw in water for more rapid absorption • Ex: IM diazepam
Oral solution: biopharmaceutics • No dissolution phase • Major concern is physicochemical stability and interaction with other substances in GI fluid • Change in pH • Dilution of cosolvent • Formation of insoluble complexes • Ciprofloxacin with Fe2+, Ca2+, Mg2+ etc. • Viscosity of solution may slow absorption • Assuming spherical drug molecule • So really, please drink a glass of water
Parenteral solutions • IV, IM, sc, intra-articular, intrathecal, etc. • Injected directly into body … unique requirements • Manufacturing (purity/sterility of components) • Preparation and admixture (asceptic technique, laminar flow hood) • Administration • “Water for Injection” (WFI) (USP 23) • Prepared by distillation or 2-stage RO • Stored and distribution at 80°C to inhibit growth • Can be stored at room temperature for <24 h • Chemical purity same as PW • Basis for many vehicles for reconstituting/diluting parenterals • NS, dextrose, Ringer’s dextrose, etc.
Sterility of parenteral solutions • Single-dose products may be preservative-free • Antimicrobials must be added to multiple-dose products • “Pharmacy bulk package” • For admixture programs thatprepare many individual doses • Used in LF hoods • Exempt from antimicrobial if<30 mL • Specially labelled
Incompatibility in admixtures • Physical • Generally precipitation due to pH change, common ion effect, insoluble salt combinations • Ex: Ca and phosphate in TPN, weak organic acids precipitating at low pH • Chemical • Covalent interactions • Ex: lactams and aminoglycosides • Therapeutic • Can be very subtle • Many incompatibilities are empiricallydetermined • Consult a reference
Containers • Grave concern for parenteral containers • Potential physical problems • Leaching • Permeation • Adsorption • Plastic containers (PVC, PE/PP copolymer) • Vials, IV bags • Permeation most significant problem • Minimize by overwrapping • Lipophilic molecules can adsorb • Ex: vitamin A, insulin • Nitroglycerin
Glass: some properties • Glass is amorphous SiO2 • Doped/contaminated withionic substances duringmanufacture • Soda (Na2CO3) • Potash (K2CO3, etc.) • Lime (CaO), etc. • Interstitial, can migrate • “Soda-lime glass” • Ions can hydrolyze ( pH) in H2O, catalyze oxidation, etc. • Glass can be attacked by solution and release glass flakes
USP classification of glass containers • Type I: borosilicate glass • Pyrex, Kimax, (Duran) • Addition of boron affords chemical (durability)and heat resistance (small dV/dT) • Suitable for all products • Type II: treated soda-lime glass • Treated with Freon or SO2 dealkalize • Greater durability • Suitable if buffered at pH <7 • Type III: soda-lime glass • For non-aqueous liquids or dry powder • Type IV: Non-parenteral (NP) • Durability determined by release of alkali released into distilled H2O under specific conditions of heat and pressure
USP: more on containers • Single-dose containers • Volume limited to <1000 mL • Multi-dose containers • Volume <30 mL (pharmacy bulk package) • Rubber septum to minimize contamination • Must also be physically compatible with solution • Same applies to connections, lines, ports, etc. • Leaching can be reduced by coating with Teflon, etc.