Download

1 / 14

E N D
1 Cleft lip and palate Cleft lip and palate Prepared by Prepared by Dr: Mohammed Alruby Dr: Mohammed Alruby رانلا كمستمف اوملظ نيلذلا ليا اونكرت لاو رانلا كمستمف اوملظ نيلذلا ليا اونكرت لاو Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
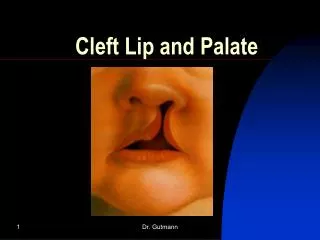
2 Cleft lip and palate Definition: Failure of union of the two palatal process with each other and with median portion of the frontonasal process at proper developmental period One of the most common congenital anomalies affecting the human craniofacial region Associated features with cleft: 1-Impaired suckling 2-Deafness 3-Sever psychological problem 4-Speech defect Incidence: Cleft lip: 1 – 4 in 1000 Cleft palate: 1 in 2000 Cleft lip: more in males than females Cleft palate: males = females Left side more than right side Unilateral more than bilateral Highest in mongoloids and Africans: 1: 500 Lowest in negroid populations: 1: 2000 In USA: 100 birth / day Development of palate: = The stomodeum is an oro-naso-pharyngeal chamber that is separated from the foregut by bucco-pharyngeal membrane, the continuity between the stomodeum and foregut is established through the rupture of the bucco-pharyngeal membrane = the frontonasal process sends a vertical extension, which divide the stomodeal cavity into two nasal cavities which form the primitive nasal septum, also sends a horizontal extension, forms the primary palate = the maxillary process develops lateral palatine shelves and at the same time the tongue was rapidly growing and completely fill the stomodeal cavity, the two palatal shelves will grow downward beside the tongue = after one week, there is a considerable enlargement of the stomodeal cavity occurs thus resulting in dropping of the tongue downward, this will free the lateral palatal shelves and so they move from vertical direction to horizontal direction, so they establish contact with each other medially and with the nasal septum superiorly and primary palate anteriorly. Thus developing the secondary palate Factors affecting normal development of palate: 1-Deficiencies of oxygen, various food stuff or vitamins 2-Endocrine disturbance 3-Some drugs and irradiation will have teratogenic effects Types of clefts: 1-Cleft lip: Unilateral: failure of maxillary prominence on affected side to unite with median nasal process Bilateral: failure of both maxillary process to unite with medial nasal process Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
3 Median upper lip: rare defect which result from mesenchymal defect which causes partial or complete formation of median nasal process Median lower lip: very rare and caused by failure of mandibular process to merge completely 2-Cleft palate: Unilateral: when one palatine shelf fails to fuse with the other components, unilateral cleft of secondary palate occurs Bilateral: if both the palatal shelves fail to fuse with each other and the midline septum, so bilateral cleft of palate occurs 3-Cleft lip and palate: Unilateral: one side of palatine process not fuse and extending into lips ULCLP Bilateral: non fusion of two palatal shelves and extending to the lips forming Y shape cleft Predisposing factors for cleft: 1-Increased maternal age: Women who with old age increased risk of having an offspring with some form of clefting, the cause unknown 2-Racial: Mongoloids show the greatest percentage 3-Blood supply: Any factor that reduce blood supply to noso-maxillary area during embryological development predispose to cleft Etiologic factors for cleft: 1-Genetic factors: a-Monogenic or single gene disorders: Half of recognized syndrome associated with cleft lip and palate are due to single gene disorder Single gene defect may give rise to Mendelian pattern of inheritance either isolated cleft lip (palate) or multiple malformation associated with cleft lip with or without palate b-Polygenic or multifactorial inheritance: Such cases show a slight familial tendency but do not conform to simple Mendelian inheritance pattern c-Chromosomal abnormalities: Chromosomal abnormalities account 18% of the clefting syndrome associated with other malformation like, Down’s (trisomy 21) or Edward (trisomy 18) 2-Environmental factors: a-Environmental teratogens: Teratogens: agent that cause congenital malformation Teratogenic drugs: -Anti-convulsion: diphenyl-hydration -Morphine overclose -Amino-protein -Alcohol consumption during first trimester – fetal alcohol syndrome -Maternal cigarette smoking -Cortisone also induce cleft palate b-Malnutrition: Folic acid defect induced by an anti-metabolic during 10 -13th day of gestation result in cleft palate in 100% of offspring Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
4 c-Infection during pregnancy: Fever and influenza are the causative organisms Toxic effect of rubella in the 1st 3 months of pregnancy associated with clefting d-Prenatal age: Women above 35 years of age had double risk of having a child with lip and palate cleft Women above 39 years of age had a triple risk of having a child with cleft palate Classification of cleft lip and palate Veau’s classification Group I: cleft soft palate only Group II: cleft of hard and soft palate, extending no further then incisive foramen, thus involving the secondary palate alone Group III: complete unilateral cleft of soft and hard palate, lip and alveolar ridge Group IV: complete bilateral cleft of soft and hard, lip and alveolar ridge on both sides ***Problems and features associated with clefts: 1-Skeletal and esthetic problems: = distorted orofacial structures = class III malocclusion = hypoplastic maxilla, concave profile 2-Dental problems: = partial anodontia: congenital missing most commonly upper laterals = presence of supernumerary teeth = enamel hypoplasia = peg shaped laterals = fused teeth = Microdontia or Macrodontia = posterior and anterior cross bite = spacing and crowding = deepbite 3-Feeding problems: Patient with cleft palate may have feeding problems due to absence of negative pressure within the oral cavity 4-Esthetic problems: Due to presence of cleft lip, there is malformation of orofacial structures and impaired the facial features Deformities of nose and nasal septum 5-Hearing and speech: = cleft lip and palate associated with middle ear disorders and frequent infections which may result in impaired hearing = the presence of hearing problem can cause difficulties in language uptake and speech Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
5 6-Psychological problems: = the parents and patient are under a lot of psychological stress = these patient may develop inferiorly complex due to their abnormal facial appearance = interaction with the community is also hindered = facing a problem with jobs and making friends Abbreviation of cleft types: = cleft lip: CL = cleft lip and alveolus: CLA = unilateral cleft lip and palate: UCLP = bifid uvula: bilateral complete lip and palate: BCLP N: B: Sub-mucous cleft: = are clinically invisible, present on the palate as bony defects but ae covered with oral mucosa = most often affect the posterior part of palate at posterior nasal spin = discovered on routine occlusal x-ray or by careful clinical palpation of palate = may occur in hard palate and continuous to open in soft palate Or in soft palate without notching the hard palate Intrauterine diagnosis: = ultrasonography and three dimensional ultrasonography enable in utero diagnosis of cleft = advantages of early diagnosis: 1-Time for parent education on the management of the baby to be born 2-Allow psychological preparation of parents and allow them to have realistic expectation 3-It gives opportunity to investigate the presence of other chromosomal abnormalities 4-Gives parent the choice of continuing the pregnancy 5-Helps in getting prepared for the neonatal feeding and care 6-Opportunity for fetal surgery Primary team for cleft patient: 1-Cleft surgeon / plastic surgeon, undertakes primary and secondary repair 2-Speech therapist, monitor speech from 9 months 3-Audiologist quantifies and locate the cause of hearing problems 4-The orthodontist monitors: Occlusion Skeletal problems Interceptive therapy Prepare for secondary alveolar graft Monitor craniofacial growth Monitor dental development Treatment results 5-Oral surgeon: secondary alveolar graft and orthognathic surgery if required 6-Plastic surgeon: correction of nose deformity, secondary deformities of lip and scar revision Other important specialist: 1-Specialist cleft nurse who can monitor the neonate during early days after birth and give feeding device 2-Clinical geneticist to resolve genetic basis of the cleft Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
6 3-Pediatric dentist to maintain health and oral hygiene 4-ENT surgeon to take care of recurrent ear infection Principles that should be followed in cleft team: 1-There should be a team leader or coordinator that facilitate the function and frequency of the team and ensure coordinated team 2-Treatment plane at any stage should be discussed by team and must follow team recommendation 3-Team must provide patient care and long term follow up Timing protocol of cleft case: 1-Palate obturation: feeding appliance: 0 month ---- 1 year 2-Primary cleft lip surgery: 3rd month 3-Palatal repair: 9 month – 1 year 4-Typansotomy tube: 6 month – 1 year 5-Speech therapy: pharyngeoplasty: 2 year – 7 year 6-Bone graft jaw: 9 year – 11 year 7-Orthodontist: 8 year – 18 year 8-Orthognathic surgery: 15 year – 18 year Management of cleft lip and palate ** Prenatal counseling: = advanced ultrasound imaging allows prenatal care and maternal fetal medicine, currently ultrasound image of cleft lip can be visualized as early as 16 weeks = when the diagnosis of cleft lip is made during pregnancy the family can referred to: 1-Prenatal consultation to explain the diagnosis 2-Review the different stages of cleft lip and palate reconstruction 3-Psychological preparation of parents for practical consideration such as feeding and social problems 4-Consultation such as geneticist to provide further discussion for associated deformities Genetic counseling: Genetic risk must be observed: == if both parents are un affected and they have affected child, the probability for their nest baby is: -If they have no affected relatives so: 4% in CL+CP -If they have an affected relative so: 2% in CP, 4% in CL+CP, 7% in CP -If the affected child has another mal-formation: 2% in CL+CP, 2% in CP = if unaffected parents have two affected children the probability for the nest baby is 9% CP+CP, and 1% CP = if one parent is affected and they have no affected children, the probability for next baby is 4% CP+CL, and 15% CP = if both parents are affected, heritability is 80% **Postnatal management of cleft lip and palate: Specific goals care for children born with cleft lip and palate include the following: 1-Minimize the feeding problems 2-Normalize the esthetic appearance of lip and nose Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
7 3-Intact primary and secondary palate 4-Normal speech, language and hearing 5-Nasal airway patency function 6-Class I occlusion with normal masticatory function 7-Good dental and periodontal health 8-Normal psychological development Stage I treatment: birth to 18 months: Passive maxillary obturator: An intra-oral device that fills the palatal cleft to: 1-Prevent escape of air, food particles and thus provide a false roofing against which child can suckle 2-Minimize feeding difficulties such as: insufficient suction, excessive air intake, nasal regurgitation 3-Prevent maxillary arch from collapsing by provide cross arch stability The obturator is fabricated using cold cure acrylic Infant orthopedics: pre-surgical orthopedics: = maxillary orthopedics was advised by Kerr Macneill in Scotland / Glasgow according to Peterson in 1947 = according to Proffit was advised by Burstone in Liverpool in late 1950 = an infant born with cleft lip and palate has distorted maxilla and pre-maxillary segment is collapsed (bilateral cases) = in unilateral cases, the distortion is not very much = this procedure was undertaken 2 -3 weeks of age 1-Collapsed posterior segment must be expanded laterally 2-Pre-maxilla must be repositioned posterior into its position in the arch, this occurs by light elastic strap across the anterior segment = pre-surgical movement indicated 3 - 6 weeks of age (Proffit) Pre-surgical movement indicated 2 - 3 weeks of age (Peterson) Latham appliance: pre-surgical orthopedic appliance Custom made acrylic appliance used for expanding and aligning the maxillary segment in patient with cleft palate Pin-retained appliance that is inserted into the palate with acrylic extension on the alveolar ridge. It has screw that is placed in cleft region and then used in manipulate the segment as desired Grayson appliance: naso-alveolar molding appliance: Used in baby with bilateral cleft Hand piece of plastic fits to the roof of the mouth. Tap is used to move and reshape the tissue segment The appliance showing vertical nasal projection that help to mold the nasal cartilages and maxillary segment Advantages of pre-surgical orthopedic and naso-alveolar molding: 1-Reduce the size of cleft and aids in surgery 2-Partial obturate the cleft and assist feeding 3-improved speech 4-places the nasal cartilages in optimal position Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
8 drawbacks of pre-surgical orthopedics: 1-add significant coast and time 2-many appliances require a general anesthetic for initial impression used to fabricate the device 3-no long term improvement in speech outcome 4-no measurable improvement in dental arc relationship was seen in patient have infant pre- surgical orthopedic device 5-frequent appointments are necessary for monitoring the anatomic change Cleft lip surgery: Surgical correction of cleft lip deformity Millard suggested the rule of 10: -10 weeks of age -10 pounds of body weight -10%mg HB blood More advantage to wait until 10-12 weeks to allow complete evaluation of any other deformities that arise at this age Surgical palate closure: May be performed in one or two operation as started with soft palate then hard palate Time of closure depend on: -Normal speech is aided by intact palate which need surgical intervention -Surgical repair of palate interferes with the normal development of maxilla Time from 10 – 12 month to 9 – 12 year Primary palate repair should be done 12 – 24 month of age and preferred in 2nd year of life Stage II treatment: 18 month to 6 year: Pharyngeal flap or; pharyngeoplasty: = 20% of children will have inadequate closure of the velopharyngeal (velopharyngeal insufficiency VPI) which may produce hyper-nasal speech = diagnosis occurs at 3 – 5 years of age Pharyngeal flap may be used to treat VPI, with goal to: 1-Improve closure between the oral and nasal cavities 2-Reduce nasal air escape during production of certain sounds Usually no active orthodontic treatment is carried out at this stage Stage III treatment: 6 – 12 year: This stage includes treatment of cross-bite and correction of maxillary retrognathism (alveolar reconstruction with bone grafting). *** orthodontic treatment in late primary or early mixed dentition: = many malocclusion features of cleft palate children result from surgical closure of lip which restrict the normal growth across the anterior part of maxillary arch = closure of palate causes some degree of lateral constriction and both anterior and posterior cross bite which is not seen in untreated cleft patient Treatment: 1-Correct upper incisors rotation and cross bite 2-Correct expansion in posterior segment 3-Prepare patient for alveolar bone graft Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
9 4-Orthodontic traction by reverse head gear 5-Put the graft between 8 – 10 years that allow eruption of lateral or canine at normal environment *** treatment of anterior and buccal cross bite: = correct the buccal cross bite is occurring firstly by using: -Split acrylic maxillary removable plate -jackscrew used to affect the force of expansion - W type of fixed expansion arch -Quad helix rapid palatal expansion and activated weekly instead of daily so the maxillary segment can effectively be expanded without breakdown of the soft tissue closure = then correct anterior cross bite: lingual locked incisors should treat by expansion Or by Z spring to avoid functional mandibular displacement and to prevent retardation of maxillary growth *** orthopedic treatment in mixed dentition: If cross bite persists: class III malocclusion can be treated by orthopedic and functional appliances like facemask therapy *** maxillary re-construction and bone grafting: = bone grafting at this site is performed during mixed dentition prior to eruption of permanent canine and / or permanent lateral incisor = indicated to restore the physiologic continuity of arch to provide bone and provide support to the lip = usually is taken up after correction of posterior and anterior cross bite Schools of graft: 1-Primary alveolar bone graft: at 18 month of age: if early grafting is not done, chances of bone loss on the surface of root lead to periodontal problem. However early grafting with lip repair and secondary palate repair produce long-term growth retardation as graft require extensive surgery 2-Secondary or delayed alveolar bone graft: 8 -10 years of age: Ideally one half to one third root should have completed Erupting tooth is a potent stimulus for bone formation as it is a functional matrix Secondary alveolar bone graft: It is interposition of bone within alveolar cleft to obliterate it, the term secondary is used when graft is put after cleft closure Types: 1-Autograft: from the same person 2-Allograft: homograft: from other person of the same species 3-Xenograft: heterograft: from member of another species Sequence and timing of cleft closure: 1-Cheilorraphy: surgical closure of lip: as medical status of infant permits most of surgeon adhere rule of 10 2-Soft palate closure: 2 years of age 3-Hard palate closure: preschool 5 -6 years of age 4-Alveolar bone graft: most surgeon prefer 7 – 10 years of age Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
10 Donner site: ribs, iliac crest, zygoma, tibia, cranial base, symphysis of mandible, some prefer rib in primary grafting Sequelae of persistence alveolar cleft: 1-Formation of oro-nasal fistula which lead to: escape of oral fluids into nasal cavity and drainage of the nasal section into the oral cavity 2-Eruption of teeth into the alveolar gap 3-Collapse of alveolar segment after surgical or orthopedic expansion 4-In case of large alveolar cleft, speech is adversely affected Advantages of alveolar bone graft: 1-Unite the alveolar segment and prevent collapse and constriction of dental arch 2-Provide bone support for teeth adjacent to cleft and for those will erupt in this area 3-Closure of oro-nasal fistula 4-Augmentation of ridge provide sufficient bone to support removable or fixed prosthesis and provide more esthetic affect to minimize unwanted look of the intra-oral bony defect 5-More support at base of nose and lip which provide normal showing of contour N: B: as a general rule, alveolar grafting should be performed before labial and nasal closure (secondary plastic surgery) Role of orthodontist related to grafting procedure: A-Before grafting: 1-In constricted maxilla: usually associated with complete alveolar and hard palate cleft: alignment of maxillary teeth as preparation for expansion also alignment of mandibular teeth 2-In case of un-constricted maxilla: usually associated with alveolar process clefts: alignment of, maxillary arch to preserve the alveolar cleft gap B-After grafting: = postoperative 3 -6 months should be allowed to permit graft uptake and bone bridging across the graft = use heavy rectangular wire with stops or un-activated open coil along the graft length = after this period, teeth can align normally through the graft with no special precautions = if canine start to erupt comes down through the graft site, wait until it erupts normally ----- then adjustment will perform if it is impacted so we can do surgical exposure and traction Maxillary expansion: A-Before grafting: -Easy -Less traumatic -High tendency for relapse which may be minimized by long period of stabilization Relapse may be due to: -Stretching of scar tissue formed as a result of primary closure of palate -Lack of bony support due to presence of cleft gap B-After grafting: Performed post-operative similar to expansion in non-cleft palate cases. Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
11 Maxillary protraction: Protraction is usually performed using facemask in combination of protraction hooks Early grafting provides early bone support of soft tissue and teeth eruption so it is better to graft before protraction. Stage IV: 12 – 18 year: With the eruption of canine and premolar teeth there is a tendency for posterior cross bite particularly at cleft side The plane of this phase is space closure, if the space closure is not possible, orthodontic tooth movement may be needed to reposition teeth as abutment Dental implants are not appropriate for cleft areas: 1-Prosthetic replacement of congenitally missing teeth 2-Correct all local irregularities like spacing, crowding and cross bite 3-Use all permanent teeth present to correct all malocclusion 4-After orthodontic treatment patient enter the retention phase which require long term permanent retention due to: Lack of bony base Congenitally Freely mobile pre-maxillary segment Presence of scar tissue from previous surgical procedure Stage V: post treatment retention: after 18 years: = orthognathic re-construction of maxillary and mandibular discrepancies is performed at 14 – 18 years = orthognathic surgery helps in correction of vertical and sagittal dimension = surgical mandibular setback also may be needed = orthognathic surgeries are performed in conjunction with the orthodontic treatment Summary of orthodontic problems with cleft lip and palate 1-Lack of bony base: Cleft lip and palate causes disruption of continuity of the maxillary arch in lateral incisors canine region and deficient alveolar bone at this region If the palate is not repaired properly, the scar tissue may constrict the alveolar arch in the transverse plane 2-Congenitally missing teeth: Children with cleft in maxilla with any severity has a higher incidence of congenitally missing teeth Commonly: Lateral incisors in cleft area Lateral incisors in contralateral incisors in cleft side Maxillary second premolars Mandibular second premolars 3-Supernumerary teeth: There is a great incidence of supernumerary teeth in cleft lip and palate patient than non-cleft populations Most common lateral incisor in maxilla at cleft side May ectopic in position and smaller in size Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
12 4-Ectopically placed teeth: Because the surgical procedure near the area of the cleft and subsequent formation of scar tissue, teeth adjacent to cleft may have deviation from path of eruption Common on lateral incisor and canine 5-Ankylosis of tooth: Sometimes, the lateral incisors and canine adjacent to area of cleft may be ankylosed, so it cannot be moved orthodontically so, extraction and prosthetic replacement should be considered 6-Other tooth anomalies: Include: fused teeth, irregularities of teeth, malformation of teeth, delayed eruption of teth due to scar tissue, 7-The freely mobile pre-maxilla: = in unilateral complete cleft, the portion of maxilla adjacent to cleft site can be positional higher than occlusal plane = in bilateral complete cleft, the pre-maxilla positioned lower than the occlusal plane, and can be rotated backward Speech problems with cleft palate 1-Retardation of consonant sounds (p, b, t, d, k, g) 2-Hyper-nasality due to soft palate cleft and may remain after surgical correction 3-Malocclusion will affect speech articulation (action of producing sounds or wards) 4-Hearing problem will adversely affect the speech process 5-All consonant except m, n, ng, will be affected 6-Unrepaired cleft lip, the sounds p, b, m, may be omitted 7-Miss placed upper anterior sounds th, f, v, z, sh, may be defective 8-Unrepaired cleft palate the sound, k, g, are omitted 9-Cleft of soft palate only: show defect on s, z, sh Hard and soft palate appeared to be superior to those with surgical closure of cleft without speech therapy E N T problems: = ENT specialist is responsible for audio-logical and otologic management of the children with clefts = Clefts may be lead to: -Disruption of tensor veli palatini muscle which play role in function of Eustachian tube --- ------ otitis media -90% of cleft patient has middle ear effusion = otitis media effusion commonly known as: glue ear ENT role: pre-scribing hearing aids Addresses issue of: -Tonsillar and adenoid hypertrophy -Sinusitis -Nasal abnormalities -Middle ear surgery of needed Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
13 Feeding problems: Due to lack of suction, an infant with cleft may have trouble in feeding Patient need special equipment for feeding such as (Haber-man feeder) Advantages of early correction of cleft: 1-Better palatal and pharyngeal muscle development once repaired 2-Ease of eating 3-Better development of phonation skill 4-Better auditory tube function 5-Better hygiene 6-Improved psychological state of patient and parents Disadvantages of early correction of cleft: 1-Surgical correction is more difficult in young children 2-Scar formation resulting in maxillary growth retardation Treatment indications At age of 6 years, patient with cleft lip and / or palate may be classified according to categories, regardless to type of clefting: Category 0: This category includes minor cleft, CL, CO and complete UCLP, and BCLP, but minimal skeletal discrepancy Need for treatment: -No need for early orthodontic treatment -Alignment of permanent incisors in the cleft area at 7 to 8 years of age -Bone grafting at 8 11 years of age -Conventional orthodontic treatment at 11 – 13 years of age Category 1: This category includes UCLP, BCLP, CP with normal skeletal facial morphology and post dental cross bite Need for treatment: -Skeletal and / or dentoalveolar transverse expansion of upper jaw -Alignment of permanent incisors in the cleft area at 7 – 8 years of age -Bone grafting at 8 – 11 years of age -Conventional orthodontic treatment at 11 to 13 years of age Category 2A: Include total UCLP and BCLP and occasionally CP with moderate skeletal facial discrepancies Need for treatment: -Interceptive orthopedics, transverse expansion and anterior protraction of upper arch at 6 – 7 years of age -Alignment of permanent incisors in the cleft area at 7 years of age -Bone grafting at 8 – 11 years of age Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby
14 -Conventional orthodontic treatment at 11 to 13 years of age Category 2B: Cannot diagnostically differentiated from category 2A until patient are 13 – 15 years of age Include total UCLP, BCLP, CP, with sever skeletal facial expression as: -Underdevelopment of upper arch -Mandibular excess ------ class III -Anterior, posterior cross bite -Vertical skeletal open bite Need for treatment: -Interceptive expansion: anterior protraction of upper arch at 6 – 7 years of age -Alignment of permanent incisors in cleft area at 7 – 8 year -Bone graft at 8 – 11 years of age -Conventional treatment at 11 – 13 years of age -Combined orthognathic and surgical correction in adulthood after completion of growth Retention and relapse = surgical scar after surgery cause relapse = Most of relapse occur in all cleft lip patients = Retention should be long time = appliance commonly used: soldered lingual retainer or Hawley retainer with pontic to replace the missing tooth if needed = expanded arches with cleft should enter long term of retention = treated patients must follow up till at least 21 years of age Cleft lip and palate Cleft lip and palate Dr. Mohammed Alruby Dr. Mohammed Alruby