Download
1 / 24
310 likes | 796 Views
Acute Respiratory Failure. Christopher B. Powe, Ph.D., ACNP Principle | Global Training Institute. Objectives. Define Respiratory Failure Discuss physiology of respiratory failure Discuss mechanisms of respiratory failure Discuss treatment of respiratory failure. Definition.

E N D
Acute Respiratory Failure Christopher B. Powe, Ph.D., ACNP Principle | Global Training Institute
Objectives • Define Respiratory Failure • Discuss physiology of respiratory failure • Discuss mechanisms of respiratory failure • Discuss treatment of respiratory failure
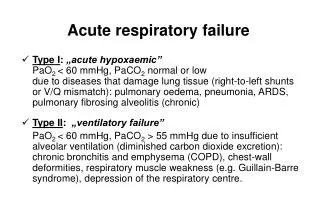
Definition • Acute Respiratory Failure (ARF) may be defined as relatively rapid respiratory dysfunction leading to acute hypoxemia and/or acute hypercapnia, severe enough to compromise the function of vital organs!!!! • A medical emergency!!!
Respiratory Failure Signs and Symptoms • Tachypnea • Dyspnea • Tachycardia • Anxiety • Diaphoresis • Coughing • Stridor • Wheezing • Rales • Accessory muscle usage • Hypoxemia • Hypocapnia or hypercapnia • Increased work of breathing • Cyanosis • Lethargy • Obtunded • Unable to speak in full sentences
General Criteria • Hypoxemia • PaO2 <55 mm Hg • Hypercapnia • PaCO2 > 50 mm Hg
Respiratory Failure • Failure of lung ventilation • Failure of lung perfusion • Failure of both ventilation & perfusion
Physiology of O2 & CO2 transport • Balance between pulmonary ventilation & capillary blood flow (V/Q) • Oxygen is bound to hemoglobin • Oxygen is limited by the amount of hemoglobin & function. • Total of 4 oxygen molecules at 4 iron binding sites • Fully saturate hemoglobin can bind 1.38 ml of O2 per gm. • Plasma can carry 0.003 times the PaO2. (1%). • CO2 diffuses into blood across the alveolar capillary membrane • Buffering is regulated by carbonic anhydrase.
Basic Causes of Hypoxemia & Hypercapnia • Low partial pressure of Oxygen • Occurs at high altitudes • Diffusion Impairment • Thickening alveolar-capillary membrane • Right-to-Left Shunt • Three types • Cardiac • Pulmonary vasculature • Pulmonary parechymal • V/Q Mismatch • Hypoventilation • Reduction in minute ventilation without underlying lung disorder • High Partial Pressure of inspired Carbon Dioxide
V/Q Shunt/Ratio • Normal V (ventilation) is 4-5 L of air per minute. • Normal Q (perfusion) is 4-5L of blood per minute. • So Normal V/Q ratio is 4/5 or 0.8 – 1.0. • When the V/Q is higher than 0.8, it means ventilation exceeds perfusion. • When the V/Q is < 1.0, there is a VQ mismatch caused by poor ventilation.
Mechanisms of Injury Hypoxemia • Anatomical • Increased permeability • Alveolar filling • Microatelectasis • Diffusion impairment • Physiologic • V/Q mismatch • R to L Intrapulmonary shunt • Decreased lung compliance (stiff) Hypercapnia: • Increased work of breathing • Respiratory muscle fatigue • Insufficient central ventilatory drive (ventilatory failure) • Impaired neuromuscular transmission of respiratory drive
Common Causes Acute Hypoxemic: • Increased permeability pulmonary edema • Noncardiogenic • Normal pressure • ARDS • Cardiogenic pulmonary edema • Normal permeability • High-pressure • Heart failure Acute Hypercapnic: • Neuromuscular disease • Trauma • Respiratory muscle fatigue • Drug overdose • Exacerbation of obstructive pulmonary disease (COPD)
Calculations for Determining Ventilation Perfusion Mismatch • Vd/Vt (dead space / Tidal Volume) • Qs/Qt • A-a PO2 Gradient • P/F Ratio • <200 ARDS • <300 ALI
Dead Space Ventilation • Anatomic dead space • Large conducting airways • 20-30% of Vt • 1-2cc per kg • Normal Vd/Vt = 0.2-0.3 • Vd/Vt = PaCO2 – PeCO2 / PaCO2 (Bohr equation) • Physiologic dead space • Airways that do not take place in gas exchange at the capillary level. • Hypercania results when Vd/Vt exceeds 0.5
Types of Intrapulmonary Shunt • True shunt • Total absence of exchange between capillary blood a alveolar gas • Venous admixture shunt • Capillary blood flow does not equilibrate with alveolar gas
Right-Left Shunt • Cardiac • Relative increase in right sided pressures • Pulmonary • Arteriovenous malformations • Parenchymal • Pneumonia, ARDS
Shunt Qs/Qt • QS/QT = (CcO2 - CaO2) / (CcO2 - CvO2) • CaCO2 = 1.39 X Hgb X SaO2 • CvO2 = ="1.39" x Hb x SvO2 + 0.003 x PvO2 • CcO2=1.39 x Hb + 0.003 x PaO2 • Shunts normal < 5%
Intrapulmonary Shunt • Small airways • Asthma, COPD • Alveoli filled with fluid • Pnumonia, pulmonary edema • Alveoli Collapsed • Atelectasis • Excessive Capillary Blood Flow • Non-embolized regions of the lung
A-a PO2 Gradient • PAO2 – PaO2 • PAO2 = FiO2 (Pb- PH2O) – (PaCO2 / RQ) • Predicted gradient = 2.5 + 0.21 X age in years • Normal gradient will increase 5-7 for each 10% increase in FiO2
Treatment • Hypoxemia • Oxygen • NBP, CPAP, FM, MV • Hypercapnia • BiPAP, MV