Download
1 / 65
850 likes | 1.72k Views
Acute Respiratory Failure. Respiratory System. Consists of two parts: Gas exchange organ (lung): responsible for OXYGENATION Pump (respiratory muscles and respiratory control mechanism): responsible for VENTILATION

E N D
Respiratory System • Consists of two parts: • Gas exchange organ (lung): responsible for OXYGENATION • Pump (respiratory muscles and respiratory control mechanism): responsible for VENTILATION NB: Alteration in function of gas exchange unit (oxygenation) OR of the pump mechanism (ventilation) can result in respiratory failure
Gas Exchange Unit Fig. 66-1
Normal ABGs • pH = 7.35-7.45 • CO2 = 35-45 • HCO3= 23-27
Respiratory and Metabolic Acidosis and Alkalosis • CO2 is an acid and is controlled by the Respiratory (Lung) system • HCO3 is an alkali and is controlled by the Metabolic (Renal) system • Respiratory response is immediate; Metabolic response can take up to 72 hours to respond (except in patients with COPD who are in a constant state of Compensation!)
ABG Interpretation Step 1: Check the pH: Is it acidotic or alkalotic or normal? pH below 7.35 is acidotic; pH above 7.45 is alkalotic If pH is normal, then the ABG is compensated; if pH not normal, then the ABG is uncompensated
ABG Interpretation (cont’d) Step 2. Check the CO2 and HCO3: • If the CO2 (acid) is above 45, the pt is acidotic; if the CO2 is below 35, the pt is alkalotic • If the HCO3 is above 27, the patient is alkalotic; if the HCO3 is below 23, the patient is acidotic
ABG Interpretation (cont’d) Step 3 If the CO2 is high (above 45), then the patient is in Respiratory Acidosis; if the CO2 is low (below 35), then the patients is in Respiratory Alkalosis. If the HCO3 is high (above 27), then the patient is in Metabolic Alkalosis; if the HCO3 is low (below 23), then the patient is in Metabolic Acidosis.
ABG Example #1 • pH = 7.36 • CO2 = 41 • HCO3 = 27 Diagnosis: ?
ABG Example #2 • pH = 7.49 • CO2 = 37 • HCO3 = 32 Diagnosis: ?
ABG Example #3 • pH = 7.29 • CO2 = 50 • HCO3 = 26 Diagnosis: ?
ABG Example #4 • pH = 7.40 • CO2 = 32 • HCO3 = 30 Diagnosis: ?
Acute Respiratory Failure • Results from inadequate gas exchange • Insufficient O2 transferred to the blood • Hypoxemia • Inadequate CO2 removal • Hypercapnia
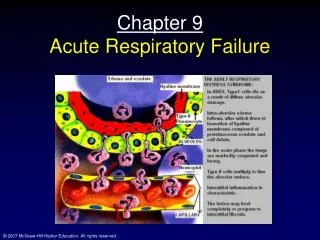
Acute Respiratory Failure with Diffuse Bilateral Infiltrates
Acute Respiratory Failure • Not a disease but a condition • Result of one or more diseases involving the lungs or other body systems • NB: Acute Respiratory Failure: when oxygenation and/or ventilation is inadequate to meet the body’s needs
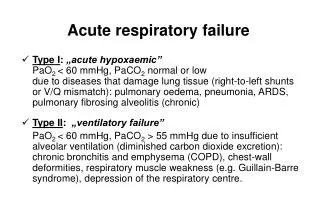
Acute Respiratory Failure • Classification: • Hypoxemic respiratory failure (Failure of oxygenation) • Hypercapnic respiratory failure (Failure of ventilation)
Classification of Respiratory Failure Fig. 66-2
Acute Respiratory Failure • Hypoxemic Respiratory Failure • PaO2 of 60 mm Hg or less (Normal = 80 - 100 mm Hg) • Inspired O2 concentration of 60% or greater
Acute Respiratory Failure • Hypercapnic Respiratory Failure • PaCO2 above normal (>45 mm Hg) • Acidemia (pH <7.35)
Hypoxemic Respiratory FailureEtiology and Pathophysiology • Causes: • Ventilation-perfusion (V/Q) mismatch • Shunt • Diffusion limitation • Alveolar hypoventilation
V-Q Mismatching I) V/Q mismatch • Normal ventilation of alveoli is comparable to amount of perfusion • Normal V/Q ratio is 0.8 (more perfusion than ventilation) • Mismatch d/t: • Inadequate ventilation • Poor perfusion
Range of V/Q Relationships Fig. 66-4
Hypoxemic Respiratory FailureEtiology and Pathophysiology Causes V/Q mismatch • COPD • Pneumonia • Asthma • Atelectasis • Pulmonary embolus
Hypoxemic Respiratory FailureEtiology and Pathophysiology II) Shunt • An extreme V/Q mismatch • Blood passes through parts of respiratory system that receives no ventilation • d/t obstruction OR fluid accumulation • Not Correctable with 100% O2
Diffusion Limitations III) Diffusion Limitations • Distance between alveoli and pulmonary capillary is one- two cells thick • With diffusion abnormalities: there is an increased distance between alveoli (may be d/t fluid) • Correctable with 100% O2
Hypoxemic Respiratory FailureEtiology and Pathophysiology Causes Diffusion limitations • Severe emphysema • Recurrent pulmonary emboli • Pulmonary fibrosis • Hypoxemia present during exercise
Diffusion Limitation Fig. 66-5
Alveolar Hypoventilation IV) Alveolar Hypoventilation Is a generalized decrease in ventilation of lungs and resultant buildup of CO2
Hypoxemic Respiratory FailureEtiology and Pathophysiology Causes Alveolar hypoventilation • Restrictive lung disease • CNS disease • Chest wall dysfunction • Neuromuscular disease
Hypoxemic Respiratory FailureEtiology and Pathophysiology • Interrelationship of mechanisms • Hypoxemic respiratory failure is frequently caused by a combination of two or more of these four mechanisms • Effects of hypoxemia • Build up of lactic acid → metabolic acidosis → cell death • CNS depression • Heart tries to compensate → ↑ HR and CO • If no compensation: ↓ O2, ↑ acid, heart fails, shock, multi-system organ failure
Hypercapnic Respiratory FailureEtiology and Pathophysiology • Imbalance between ventilatory supply and demand • Occurs when CO2 is increased
Causes Hypercapnic Respiratory Failure I) Alveolar Hypoventilation and VQ Mismatch: • Ventilation not adequate to eliminate CO2 • Leads to respiratory acidosis • Eg. Narcotic OD; Guillian-Barre, ALS, COPD, asthma
Causes Hypercapnic Respiratory Failure II) VQ Mismatch: - Leads to increased work of breathing - Insufficient energy to overcome resistance; ventilation falls; ↑PCO2; respiratory acidosis
Hypercapnic Respiratory FailureCategories of Causative Conditions • I) Airways and alveoli • Asthma • Emphysema • Chronic bronchitis • Cystic fibrosis
Hypercapnic Respiratory FailureCategories of Causative Conditions • II) Central nervous system • Drug overdose • Brainstem infarction • Spinal cord injuries
Hypercapnic Respiratory FailureCategories of Causative Conditions • III) Chest wall • Flail chest • Fractures • Mechanical restriction • Muscle spasm
Hypercapnic Respiratory FailureCategories of Causative Conditions • IV) Neuromuscular conditions • Muscular dystrophy • Multiple sclerosis
Respiratory FailureTissue Oxygen Needs • Major threat is the inability of the lungs to meet the oxygen demands of the tissues
Respiratory FailureClinical Manifestations • Sudden or gradual onset • A sudden in PaO2 or rapid in PaCO2 is a serious condition
Respiratory FailureClinical Manifestations • When compensatory mechanisms fail, respiratory failure occurs • Signs may be specific or nonspecific
Respiratory FailureClinical Manifestations • Severe morning headache • Cyanosis • Late sign • Tachycardia and mild hypertension • Early signs
Respiratory FailureClinical Manifestations • Consequences of hypoxemia and hypoxia • Metabolic acidosis and cell death • Cardiac output • Impaired renal function
Respiratory FailureClinical Manifestations • Specific clinical manifestations • Rapid, shallow breathing pattern • Sitting upright • Dyspnea
Respiratory FailureClinical Manifestations • Specific clinical manifestations • Pursed-lip breathing • Retractions • Change in Inspiratory:Expiratory ratio
Respiratory FailureDiagnostic Studies • Physical assessment • ABG analysis • Chest x-ray • CBC • ECG
Respiratory FailureDiagnostic Studies • Serum electrolytes • Urinalysis • V/Q lung scan • Pulmonary artery catheter (severe cases)
Acute Respiratory FailureNursing and Collaborative Management • Nursing Assessment • Past health history • Medications • Surgery • Tachycardia