Download
1 / 28
310 likes | 996 Views
RESPIRATORY FAILURE AND ACUTE RESPIRATORY DISTRESS SYNDROME. Fadi J. Zaben RN MSN IMET2000, Ramallah. RESPIRATORY FAILURE. RESPIRATORY FAILURE:. Respiratory failure is an alteration in the function of the respiratory system.

E N D
RESPIRATORY FAILUREAND ACUTE RESPIRATORY DISTRESS SYNDROME Fadi J. Zaben RN MSN IMET2000, Ramallah
RESPIRATORY FAILURE: • Respiratory failure is an alteration in the function of the respiratory system. • Partial pressure of arterial oxygen (Pao2) to fall below 50 mm Hg (hypoxemia). • And/or the partial pressure of arterial carbon dioxide (Paco2) to rise above 50 mm Hg (hypercapnia). • Respiratory failure is classified as acute, chronic, or combined acute and chronic.
Classification: • Acute Respiratory Failure • Chronic Respiratory Failure. • Acute and Chronic Respiratory Failure.
Acute Respiratory Failure: • Characterized by: • Hypoxemia (Pao2 less than 50 mm Hg). • Hypercapnia (Paco2 greater than 50 mm Hg). • Acidemia (pH less than 7.35). • Occurs rapidly, usually in minutes to hours or days.
Chronic Respiratory Failure: • Characterized by: • Hypoxemia (decreased Pao2). • Hypercapnia (increased Paco2). • Normal pH (7.35 to 7.45). • Occurs over a period of months to years allows for activation of compensatory mechanisms.
Acute and Chronic Respiratory Failure: • Characterized by: increase in the degree of hypoxemia or hypercapnia in patients with preexisting chronic respiratory failure. • May occur after an acute upper respiratory infection or pneumonia, or without obvious cause. • Extent of deterioration is best assessed by comparing the patient's present ABG levels with previous ABG levels.
Clinical Manifestations: • Hypoxemia restlessness, agitation, dyspnea, disorientation, confusion, delirium, loss of consciousness. • Hypercapnia headache, dizziness, and confusion. • Tachypnea initially; then when no longer able to compensate, bradypnea. • Accessory muscle use. • Asynchronous respirations.
Diagnostic Evaluation: • ABG analysis: show changes in Pao2, Paco2, and pH from patient's normal; or Pao2 less than 50 mm Hg, Paco2 greater than 50 mm Hg, pH less than 7.35. • Pulse oximetry: decreasing Sao2. • End tidal CO2 monitoring: elevated. • Complete blood count, serum electrolytes, chest X-ray, urinalysis, electrocardiogram (ECG), blood and sputum cultures; to determine underlying cause and patient's condition.
Management: • Oxygen therapy to correct the hypoxemia. • Chest physical therapy and hydration to mobilize secretions. • Bronchodilators and possibly corticosteroids to reduce bronchospasm and inflammation. • Diuretics for pulmonary congestion. • Mechanical ventilation as indicated. Noninvasive positive-pressure ventilation using a face mask may be a successful option for short-term support of ventilation.
Complications: • Oxygen toxicity if prolonged high Fio2 required. • Barotrauma from mechanical ventilation intervention
Nursing Assessment: • Note changes suggesting increased work of breathing (tachypnea, diaphoresis, intercostal muscle retraction, fatigue) or pulmonary edema. • Assess breath sounds (diminished or absent sounds, crackles, wheezing, rhonchi and crackles ). • Assess level of consciousness (LOC) and ability to tolerate increased work of breathing. • Assess for signs of hypoxemia and hypercapnia. • Analyze ABG and compare with previous values. • Determine hemodynamic status (blood pressure, cardiac output)
Nursing Diagnoses: • Impaired Gas Exchange related to inadequate respiratory center activity or chest wall movement, airway obstruction, and/or fluid in lungs • Ineffective Airway Clearance related to increased or tenacious secretions
:Nursing Interventions • Improving Gas Exchange: • Administer antibiotics, cardiac medications, and diuretics as ordered for underlying disorder. • Administer oxygen. • Monitor fluid balance by intake and output measurement, urine specific gravity, daily weight to detect presence of hypovolemia or hypervolemia. • Provide measures to prevent atelectasis and promote chest expansion and secretion clearance, as ordered (incentive spirometer, nebulization, head of bed elevated 30 degrees, turn frequently, out of bed). • Monitor ABG levels.
Patient Education and Health Maintenance: • Instruct patient with preexisting pulmonary disease to seek early intervention for infections to prevent acute respiratory failure. • Teach patient about medication regimen: • Proper technique for inhaler use. • Dosage and timing of medications. • Monitoring for adverse effects of corticosteroids: weight gain due to fluid retention, polyuria and polydipsia due to hyperglycemia, mood changes.
Acute Respiratory Distress Syndrome: • ARDS is a clinical syndrome also called noncardiogenic pulmonary edema. • It is a life-threatening lung condition that prevents enough oxygen from getting into the blood. • It is severe hypoxemia and decreased compliance of the lungs. • It leads to both oxygenation and ventilatory failure. • Mortality is 50% to 60% but is improved with early intervention.
Pathophysiology and Etiology: • Pulmonary and/or nonpulmonary insult to the alveolar-capillary membrane causing fluid leakage into interstitial spaces. • Ventilation-perfusion mismatch caused by shunting of blood.
……. Continue • Etiologies are numerous and can be pulmonary or nonpulmonary. These include: • Pneumonia, sepsis, aspiration. • Shock (any cause), trauma. • Metabolic, hematologic, and immunologic disorders. • Inhaled agents smoke, high concentration of oxygen, corrosive substances. • Major surgery, fat or air embolism.
Clinical Manifestations: • Symptoms usually develop within 24 to 48 hours of the original injury or illness. • Severe dyspnea, use of accessory muscles. • Increasing requirements of oxygen therapy. Hypoxemia refractory to supplemental oxygen therapy. • Severe crackles and rhonchi heard on auscultation.
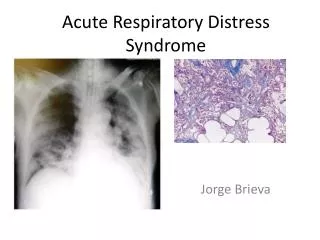
Diagnostic Evaluation: • The hallmark sign for ARDS is a shunt; hypoxemia remains despite increasing oxygen therapy. • Decreased lung compliance; increasing pressure required to ventilate patient on mechanical ventilation. • Chest X-ray exhibits bilateral infiltrates.
Treatment: • The treatment for ARDS is aimed at symptom management, but the underlying cause must be treated or the ARDS will not resolve. • Supportive measures will assist the patient while the underlying cause is being treated. • The underlying cause for ARDS must be determined so appropriate treatment can be initiated.
Continue……… • Ventilatorysupport and low oxygen therapy concentration. • Fluid management must be maintained. • Medications are aimed at treating the underlying cause. • Corticosteroids are used infrequently due to the controversy regarding benefits of usage. • Adequate nutrition should be initiated early and maintained.
Complications: • Infections, such as pneumonia, sepsis. • Respiratory complications, such as pulmonary emboli, barotrauma, oxygen toxicity, subcutaneous emphysema, or pulmonary fibrosis. • GI complications, such as stress ulcer, ileus. • Cardiac complications, such as decreased cardiac output and dysrhythmias. • Renal failure, disseminated intravascular coagulation.
Prognosis: • A third of people with ARDS die from the disease. • Many people have permanent (usually mild) lung damage. • Many people who survive ARDS have memory loss or other quality-of-life problems after they recover.
Prevention: • The only way to prevent ARDS is to avoid those diseases and harmful conditions that damage the lung. • For instance, the danger of aspirating stomach contents into the lungs can be avoided by making sure a patient does not eat shortly before receiving general anesthesia. • If a patient needs oxygen therapy, as low a level as possible should be given. • Any form of lung infection, or infection anywhere in the body that gets into the blood, must be treated promptly to avoid the lung injury that causes ARDS.
Nursing Interventions: Nursing Care is similar to patient with respiratory failure.