Download
1 / 13

E N D
Acute respiratory failure • Type I:„acute hypoxaemic” PaO2 < 60 mmHg, PaCO2 normal or low due to diseases that damage lung tissue (right-to-left shunts or V/Q mismatch): pulmonary oedema, pneumonia, ARDS, pulmonary fibrosing alveolitis (chronic) • Type II:„ventilatory failure” PaO2 < 60 mmHg, PaCO2 > 55 mmHg due to insufficient alveolar ventilation (diminished carbon dioxide excretion): chronic bronchitis and emphysema (COPD), chest-wall deformities, respiratory muscle weakness (e.g. Guillain-Barre syndrome), depression of the respiratory centre.
Clinical assessment of respiratory distress • The use of accessory muscles of respiration • Tachypnoe • Tachycardia • Sweating • Pulsus paradoxus • Inability to speak • Signs of CO2 retention (peripheral vasodilation, a bounding pulse, a coarse flapping tremor, confusion, progressive drowsiness, coma, papilloedema) • Asonchronous respiration • Paradoxical respiration
Gas blood analysis pH 7.35-7.45 PaO2 75-100 mmHg PaCO235-45 mmHg HCO3- 21-28 mmHg HCO3- pCO2 Saturation vs. oxygenation SaO2 PaO2 pulse oximetry
Management of respiratory failure – I.C.U. • Oxygen therapy • Respiratory support (e.g. IPPV, CPAP, IMV, HFJV). • Control of secretions • Treatment of pulmonary infection • Control of airways obstruction • Limitation of pulmonary oedema
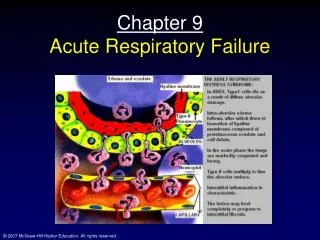
ARDS = adult respiratory distress syndrome Syndrome of severe dyspnoea, tachypnoea, cyanosis refractory to oxygen therapy, a reduction in lung compliance (stiff lungs), diffuse alveolar infiltrates on the chest X-ray Causes: sepsis, shock, fat embolism, trauma, burns, acute pancreatitis, inhalation of smoke and toxic gases, amniotic fluid aspiration... usu. a part of MOF Mortality: > 50% overall
Chronic respiratory failure • COPD = chronic obstructive pulmonary disease, a condition of chronic obstruction to airflow due to: • Chronic bronchitis(cough with expectoration for at least 3 months of the year for more than 2 consecutive years). • Emphysema(permanent, abnormal distension of the air spaces distal to the terminal brochiole with destruction of alveolar septa). • Clinical picture: • „blue bloater” vs. „pink puffer”
Pleural disease • Dry pleurisy • Pleural effusion • Chylothorax • Empyema – complication of pneumonia • Pneumothorax • Malignancy
Exsudate vs. transsudate – laboratory features • Light’s criteria: exsudate when 1 criterion is present: • fluid protein/serum protein > 0.5 • fluid LDH/serum LDH > 0.6 • fluid LDH > 2/3 of upper normal value in serum
Pleural fluid examination • appearance • protein and LDH content • cellular content (lymphocytosis malignancy, TBC) • pH (if 7.2 drainage of infected fluid is necessary) • glucose (< 3.3 mmol/l: RA, empyema) • amylase • cytology • bacterial culture • TBC
Pneumothorax • Trauma • Chronic bronchitis, emphysema • Spontaneous: tall and thin young males, M:F = 6:1, both lungs are effected with equal frequency • Lung carcinoma • Bronchial asthma
Pneumothorax - management • Chest X-ray on expiration • Small pneumothorax: < 20% of radiographic volume: observe, avoidance of strenous exercise • Medium (20-50%): aspiration, intercostal drainage with underwater seal • Large (> 50%, shift of trachea and mediastinum): as above • Tension pneumothorax • Recurrent pneumothorax (more than twice): surgery (pleurectomy), talc pleurodesis.