Download
1 / 35
390 likes | 1.1k Views
Chapter 9 Acute Respiratory Failure. Topics. Acute respiratory failure pathophysiology Hypoxemia Co 2 retention Diaphragmatic failure Types of respiratory failure. Case Study #9: Ivan. 45 yr old computer programmer Well until 10 days ago Car accident

E N D
Topics • Acute respiratory failure • pathophysiology • Hypoxemia • Co2 retention • Diaphragmatic failure • Types of respiratory failure
Case Study #9: Ivan • 45 yr old computer programmer • Well until 10 days ago • Car accident • Multiple fractures and lung contusion • Very SOB, in and out of consciousness
Physical exam #9: Ivan • 2cd day exam • ill, with obvious dyspnea • Temp: 38.5 °C • BP: 125/60 • Pulse: 110 • Poor breath sounds • No edema
Investigations • Blood counts normal • Grossly abnormal chest radiograph • Whiteout pattern • Alveolar exudate or edema • Blood gases • Po2: 51 • Pco2: 45 • pH: 7.35 • Diagnosis: Acute respiratory failure (due to trauma) • Treatment • Intubated and mechanically ventilated (40% O2) • Swan Ganz catheter inserted in RA (CVP) • Patient died on 7th day
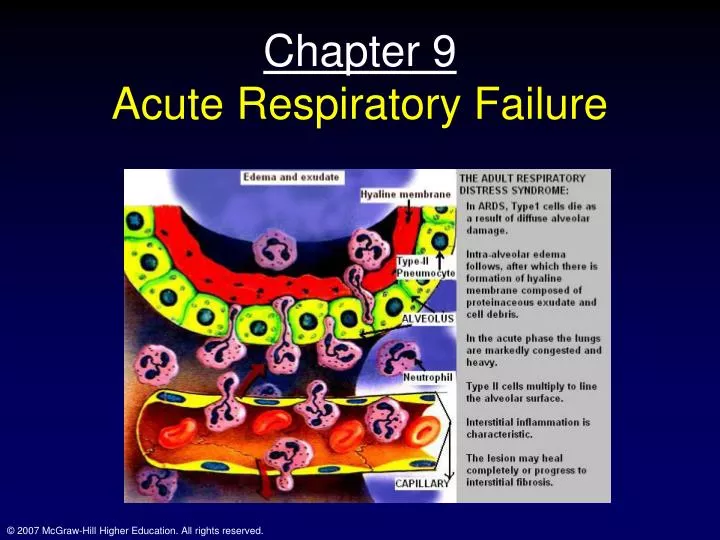
Pathophysiology • Also called ARDS (Adult respiratory distress syndrome) • Respiratory failure • When lungs fail to oxygenate the blood or prevent Co2 retention • Gas exchange • Hypoxemia and hypercapnia • Fig. 9-3 Fig. 9-3
Pathophysiology: gas exchange • Fig. 9-3 • I to A • Pure hypoventilation • Increase in Pco2 can be predicted by alveolar ventilation eq • This pattern occurs in some diseases and narcotic overdose • normal to B • Severe VA/Q mismatch • Resp failure of COPD • O2 therapy results in B to F (there resp drive is driven by hypoxemia)
Physiology and Pathophysiology of gas exchange • Normal to C • Severe interstitial lung disease • Severe hypoxemia but no hypercapnia due to hyperventilation • Normal to D • Some ARDS patients • So they follow D to E with O2 therapy
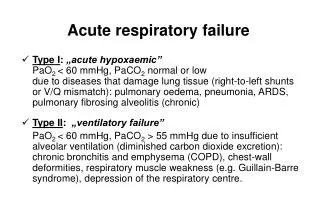
Hypoxemia of Respiratory Failure • Four mechanisms of hypoxemia • Hypoventilation • Diffusion impairment • Shunt • VA/Q mismatch • Respiratory failure • All can contribute • VA/Q mismatch most important
Hypoxemia • Mild hypoxemia • Few physiologic problems • Po2 of ~ 60 mmHg still about 90% saturation • When Po2 falls below 40-50 mmHg • CNS vulnerable • Headache, somnolence, clouding of consciousness
Hypoxemia • Tachycardia • SNS activity increased • Heart failure • If heart disease is present • Renal function impaired • Pulm hypertension • Due to hypoxic VC • Tissue hypoxia • Major culprit here • Increased anaerobic metabolism causes fall in pH
Carbon dioxide Retention • Two mechanisms • Hypoventilation • Pco2 = Vco2/VA • VA/Q mismatch • Inefficient gas exchange • Release of hypoxic VC due to high O2 therapy • Some patients depend on hypoxic ventilatory drive; despite mild hypercapnia • Thus, lower O2 concentration (just enough to raise PaO2) • Co2 retention • Increases cerebral BF • Headache, elevated CSF pressure
Acidosis of resp failure and diaphragm fatigue • Acidosis • Co2 retention • Metabolic acidosis • Diaphragm fatigue • Due to prolonged elevations in work of breathing • Hypoventilation • Co2 retention • Sever hypoxemia
Types of respiratory failure • Acute overwhelming lung disease • Bacterial or viral pneumonia • Pulm embolism • Exposure to toxic gases (chlorine, nitrogen oxides) • Neuromuscular disorders • Causes • 1) depression of breathing centers (drugs) • 2) diseases of medulla (encephalitis, trauma, hemorrhage) Fig 9-4
Types of respiratory failure • 3) Abnormal spinal conduction pathways • High cervical dislocation • 4) Anterior horn disease • Polio • 5) Disease of nerves to respiratory musculature • Guillain-Barre syndrome • 6) Diseases of neuromuscular junction • Myashtenia gravis and anticholinesterase poisoning
Types of respiratory failure • 7) Diseases of respiratory musculature • Muscular dystrophy • 8) Thoracic cage abnormalities • Crushed chest • 9) Upper airway obstruction • Tracheal compression • Essential features • Hypoventilation • Co2 retention • Hypoxemia • Respiratory acidosis
Acute or Chronic lung disease • Contains those pts with • Chronic bronchitis, emphysema, asthma and cystic fibrosis • Those with COPD have slow downhill slide • Increasingly severe hypoxemia and hypercapnia over the years • Infection usu, pushes these pts over the edge
Acute Respiratory Distress Syndrome • Acute respiratory failure • Many causes • Trauma • Aspiration • Sepsis • Shock • Early • Interstitial and alveolar edema • Hemorrhage, debris in alveoli, atelectasis • Later • Hyperplasia • Damaged alveolar epithelium becomes lined with type II alveolar cells
Acute respiratory distress syndrome • Pathogenesis • Unclear • Damage to type I cells • Accum. Of neutrophils • Cause release of histamine, bradykinin and platelet activating factor • Oxygen radicals and cyclooxygenase products (thromboxane, leukotrienes and prostaglandins • Pulm function • Impaired • Lungs become stiff • Severe VA/Q mismatch • Maybe 50% low VA/Q
Infant Respiratory Distress Syndrome • Much in common with ARDS • Hemorrhagic edema • Atelectasis • Fluid and debris in alveoli • Profound hypoxemia • High degree of VA/Q inequality • May also have R to L shunt (foramen ovale)
IRDS • Chief cause • Lack of surfactant • Surfactant system matures late in fetal life • Check lecithin/sphingomyelin ratio of amniotic fluid • Treatment • Instillation of surfactant
Oxygen therapy • Response depends on cause of hypoxemia • Hypoventilation • Small increases in PiO2 work very well • PAO2 = PiO2 –[PaCO2/R] • PaO2 increases about 1 mmHg per mmHg increase in PiO2 • Diffusion impairment • O2 also very effective • Increases driving pressure
Oxygen therapy • VA/Q mismatch • O2 administration can be effective • Cautions • If regions of the lung are poorly ventilated (low VA/Q); takes a while to wash out the N2 and raise the PAO2 • Oxygen therapy may cause poorly ventilated areas to become non-ventilated (due to collapse); shunt
Oxygen therapy • Shunt • Does not respond well to Oxygen therapy • Blood bypasses ventilated alveoli and does not benefit from the additional PAO2 • Thus, 100% is a good way to detect shunt; how? • However, may raise PaO2 enough • Dissolved Po2 can rise from 0.3 to 1.8 ml/dl (PAO2 increase from 100 to 600) • Note increase in PaO2 for person with 30% shunt (PaO2 from 55 to 110; increases SaO2 by about 10%)
Oxygen delivery: other factors • Hemoglobin conc., position of O2-Hb diss. Curve, Qc, distribution of blood flow • Both [Hb] and Qc effect O2 delivery (QO2) in the following way • Qo2 = Qc X CaO2 • CaO2 = 1.39 x [Hb] x SaO2 (%) + dissolved
Position of O2-Hb curve and blood flow distribution • Rearrangemnt of the Fick eq. yields the following • CvO2 = CaO2 –[Vo2/Qc] • Or • PcapO2 = PaO2 –[mVo2/Qm] • Thus, CvO2 and PcapO2 fall if Cao2 (PaO2) or Qc falls • CaO2 – Po2 relationship depnds on position of O2-Hb curve • Curve is shifted to the right by chronic hypoxemia (2,3 DPG)
Hazards of O2 therapy • CO2 retention • In those with Hypoxic drive • Give lower O2 conc • 24-30% • O2 toxicity • High O2conc over time can damage lung • Swollen cap endothelium, replacement of alveolar type I with type II cells, edema; long-term: fibrotic changes
Atelectasis • Following airway occlusion • 100% O2 and mucus plug • Note the great diff in total pressure when 100% O2 is breathed (due to N2 washout) • This predisposes the alveoli to collapse as gas leaves to equalize pressure • Will happen in air breathing and mucus plug, but process is slower
Atelectasis • Nitrogen is thus important in keeping alveoli open • Closure occurs in bottom of lung (less well expanded) • Secretions tend to collect at the base as well • Instability of units with low VA/Q
Atelectasis • Lung units with low VA/Q become unstable when high O2 is inhaled • Poorly ventilated areas collapse • Air in much great than expired (taken up by blood)
Patterns of ventilation • PEEP • Positive end-expiratory pressure • Improves PaO2 in Acute resp diesease • Why? • Increases FRC • Reduces airway closure • Reduces shunt • Minimizes the VA/Q mismatch • Increases VD • Compression of capillaries • Increases conducting zone volume (as consequence of inc. lung vol)
PEEP • Note the difference in the capillary volume with PEEP • PEEP also reduces Qc • Impedes venous return • Can damage capillaries • Pulmonary edema • High lung volume can cause pulm cap stress failure
Other diseases • Pneumonia • Inflammation of lung parenchyma • Alveoli fill with exudate • Can be lobar or patchy (bronchopneumonia) • Shunting and hypoxemia occur
Other diseases • Tuberculosis • Infection (bacterial) • Usu. Found in apices due to high VA/Q and high Po2 • Antibiotics: primary treatment • Old treatment? • Bronchiectasis • Dilation of Bronchi with suppuration • Pus present, due to bacterial infection (sometimes following pneumonia) • Antibiotics • Cystic Fibrosis • Disease of exocrine glands caused by abnormal chloride and sodium transport • Excessive secretions in lung (hypertrophied mucus glands)
Other pneumoconioses • Coal worker’s lung • Massive fibrosis • Silicosis • Inhalation of silica • Quarrying, mining or snadblasting • These are toxic particles • Provoke severe fibrosis • Asbestos-related disease • Commonly used in insulation, brake linings, roofing materials (anything that must resist heat • Diffuse interstitial pulm fibrosis (Chpt 5) • Bronchial carcinoma; aggravated by smoking • Pleural disease; malignant mesothelioma (sometimes up to 40 yrs after exposure) • Byssinosis • Cotton dust • Histamine reaction • Obstructive disease pattern • Occupational asthma • Allergenic organic dusts • Flour; wheat weevil • Gum acacia • Polyurethane; Toluene diisocyanate