Download
1 / 45
450 likes | 997 Views
Dermatitis 101: Diagnosis and Treatment of Eczema. Adrian Guevara MD. Dermatitis 101. Atopic Seborrheic Contact Allergic Irritant Nummular Asteatotic Stasis Neurodermatitis/Lichen Simplex Chronicus. Dermatitis 101. Dermatitis=“Eczema”=Spongiosis. Dermatitis 101.

E N D
Dermatitis 101:Diagnosis and Treatment of Eczema Adrian Guevara MD
Dermatitis 101 • Atopic • Seborrheic • Contact • Allergic • Irritant • Nummular • Asteatotic • Stasis • Neurodermatitis/Lichen Simplex Chronicus
Dermatitis 101 Dermatitis=“Eczema”=Spongiosis
Dermatitis 101 Acute Dermatitis
Dermatitis 101 Subacute Dermatitis Commonly misdiagnosed as tinea
Dermatitis 101 Chronic Dermatitis Commonly misdiagnosed as psoriasis
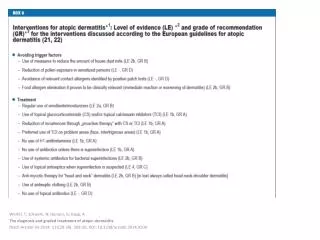
Allergic Contact Dermatitis • Type 4 Hypersensitivity Response • Classically well demarcated/patterned • Exposure can be infrequent (once a month) • Patch testing is gold standard for diagnosis • Severe reactions need systemic steroids Forget the dose pack
Allergic Contact Dermatitis • Poison Ivy/Oak/Sumac linearity
Allergic Contact Dermatitis • Potassium Dichromate in Leather
Allergic Contact Dermatitis • Latex • Cleaning products • Cosmetics • Occupational exposures Check the feet and nails!!!
Irritant Contact Dermatitis • Most contact dermatitis is irritant in nature • Occupational morbity • Irritant vs allergic • Prevention is key!
Lip licker dermatitis Blunting of vermillion Accentuation of angles
Atopic Dermatitis • 10-20% of population • Primary symptom: itch • Location, location, location • Associated with atopic background Periorbital pallor
52 y/o male with erythematous, scaly patches of face and scalp
Seborrheic Dermatitis • Distribution • Face, scalp, axillae, upper chest • Chronic condition • Nonsteroidal adjuvants • Disease associations
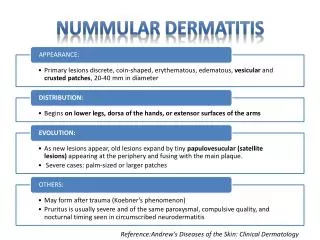
Nummular Dermatitis • Coin shaped patches and plaques • Secondary to xerosis cutis • Primary symptom itch Notice the surrounding xerosis
Asteatotic Dermatitis • Extreme case of xerosis • Riverbed type cracking
Stasis Dermatitis • Venous hypertension • Full spectrum of timing • Id reaction common • Complicated by ulceration
Lipodermatosclerosis Pseudokaposi’s (acroangiodermatitis) Venous ulceration Dispigmentation (chronic)
Id reaction Superimposed allegic contact Do: 1) dry weeping lesions 2) cover for infection Don’t: 1) apply neosporin 2) just hope steroids will fix it
Neurodermatitis/Lichen Simplex Chronicus • Paroxysmal pruritus • Habitual excoriating or rubbing • Skin thickens to defend • Consider underlying disease Increased skin markings
Lichen simplex chronicus No fungus on the scrotum! Prurigo simplex
Butterfly sign Prurigo Nodularis Consider screening
Prevention • Remove the offending agent • Edema, allergen, irritant, yeast, long fingernails • Daily cleansing and MOISTURIZING • Dove, Oil of Olay, Neutrogena • Mild temperatures • Cream/Ointment based emollients Neosporin, antifungals ≠ moisturizers
Treatment • Topical Steroids • Clobetasol I • Triamcinolone IV • Desonide VI • Hydrocortisone VII
Treatment • TIM • Protopic 0.1% oint • Elidel cr • Light • nbUVB • Systemic immunosuppressives • Prednisone • Cyclosporine • Azathioprine • IVIG Only on thin skin !!!
Treatment • Antihistamines • Mechanism of action: soporific Indications for Dermatitis ≠ Urticaria
Common Pitfalls • Misdiagnosis • Scabies (intensely pruritic, burrows/vesicles, others itch) • Psoriasis (elbows/knees/inflammatory arthritis/nail changes) • Fungus (central sparing, well marginated, scaly border) Lose the Lindane!
25 y/o male tx’d for eczema in antecubital fossa with “some cream”
Common Pitfalls • Mistreatment • Lose the Lotrisone! • 1) Commit to a diagnosis • 2) Shotgunners: “Don’t be a wimp” • Quadriderm: betamethasone, gentamycin, clotrimazole • Animax