Download
1 / 15
150 likes | 259 Views
The PRIMIS Comparative Analysis for Coronary Heart Disease. Dr Pete Horsfield PRIMIS Clinical Director. Outline. Rationale for the queries Issues emerging during authoring Issues emerging from feedback Strengths and weaknesses. NSF for Coronary Heart Disease.

E N D
The PRIMISComparative Analysis for Coronary Heart Disease Dr Pete Horsfield PRIMIS Clinical Director
Outline • Rationale for the queries • Issues emerging during authoring • Issues emerging from feedback • Strengths and weaknesses
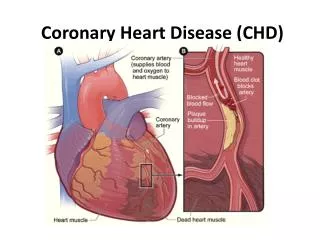
NSF for Coronary Heart Disease PREVENTING coronary heart disease The people most likely to benefit from treatments are those at greatest risk of a cardiovascular event. These are also the people in whom treatment is most cost-effective. People who have already had a heart attack, have angina or who have undergone coronary revascularisation are at particularly high risk. Identifying and treating those at greatest risk is one of the highest priorities of this NSF.
NSF standards • Reducing heart disease in the population (1 & 2) • Preventing CHD in high risk patients (3 & 4) • Heart attack and other acute coronary syndromes (5, 6 & 7) • Stable angina (8) • Revascularisation (9 & 10) • Heart failure (11) • Cardiac rehabilitation (12)
NSF standards • Reducing heart disease in the population(1 & 2) • Preventing CHD in high risk patients(3 & 4) • Heart attack and other acute coronary syndromes(5, 6 & 7) • Stable angina(8) • Revascularisation(9 & 10) • Heart failure(11) • Cardiac rehabilitation(12)
NSF for Coronary Heart Disease • People who have: • Established heart disease • Other occlusive arterial disease (OAD) • occlusive stroke • transient ischaemic attack (TIA) • peripheral vascular disease (PVD) • Multiple risk factors for heart disease are typically three to five times more likely to die, suffer a heart attack or other major cardiovascular event than people without such conditions or risk factors.
PRIMIS CHD query sets • Basic • CHD as a global entity • Prevalence, incidence • Drug interventions • Aspirin, statins, neither, both • Contraindications, refusals, etc. • Process data • OAD, AF, heart failure • with CHD, without CHD • Hypertension, diabetes • with CHD, without CHD
PRIMIS CHD query sets • Intermediate • MI and Angina as discrete groups • Prevalence, incidence • Drug interventions • Aspirin, statin, beta blocker, ACE, all, none • Contraindications, refusals, etc. • Process data • Non-CHD • Screening data • Risk factors
PRIMIS CHD query sets • Advanced • AF, stroke disease, heart failure, PVD as discrete groups • Prevalence, incidence • Drug interventions • Aspirin, warfarin, statins, ACE • Contraindications, refusals, etc. • Process data • Intermediate outcomes • BP, cholesterol • MI and Angina groups also
Issues • What’s in a code? • The art of the possible • Who wants to know?
What’s in a code – Occlusive arterial disease? Used? Should be? G71 cerebral haemorrhage no no G711 subarachnoid haemorrhage yes no G712 intracerebral haemorrhage yes no G713 extradural haemorrhage no no G714 subdural haemorrhage no no G71Z cerebral haemorrhage NOS no ?yes G72 precerebral arterial occlusion yes yes G721 basilar artery occluded yes yes G722 carotid artery occluded yes yes G723 vertebral artery occluded yes yes G72Z precerebral arterial occlusion NOS yes yes G73 cerebral arterial occlusion yes yes G731 cerebral thrombosis yes yes G732 cerebral embolism yes yes G73Z cerebral arterial occlusion NOS yes yes G74 transient cerebral ischaemia yes yes G75 stroke/CVA undefined yes yes G76 other cerebrovascular disease no no G761 cerebral arteriosclerosis no yes G762 hypertensive encephalopathy no yes G763 cerebral aneurysm-non-ruptured no no G76Z other cerebrovascular disease NOS no ?yes G77 cerebrovascular disease late effects no yes G78 Binswanger’s disease (subcortical arteriosclerotic encephalopathy) no ?yes G7Z cerebrovascular disease NOS no ?yes
The art of the possible • Beta blockade post MI • 1 year? • 2 years? • Lifelong? • “Beta-blockers (to be continued for at least one year)” • Obstacles • MIQUEST capabilities • User practice
The art of the possible (2) • Incidence data • How else to monitor outcome?
Who wants to know? • Measuring achievement • Supporting improvement • Identifying opportunities • Rush for practices • Iterative process • Invite feedback • Review product