Download
1 / 34
410 likes | 784 Views
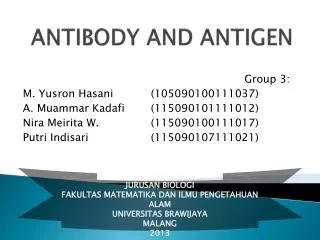
Antibody Isotypes, Idiotypes, and Allotypes. W. Robert Fleischmann, Ph.D. Department of Urologic Surgery University of Minnesota Medical School rfleisch@umn.edu (612) 626-5034. Objectives. Understand the terms isotypes, idiotypes, and allotypes of antibodies

E N D
Antibody Isotypes, Idiotypes, and Allotypes W. Robert Fleischmann, Ph.D. Department of Urologic Surgery University of Minnesota Medical School rfleisch@umn.edu (612) 626-5034
Objectives • Understand the terms isotypes, idiotypes, and allotypes of antibodies • Understand the major characteristics of each isotype and their biologic functions • Understand the biological and medical significance of idiotype and anti-idiotype antibodies
Billy Daniels, age 8 months, is brought to the clinic by his parents for testing. While he is healthy at this moment, for the past 3 months, Billy has had a series of bouts of pneumonia caused by Streptococcus pneumoniae and Haemophilus influenzae (type b). He has contracted these infections despite the fact that he has had the recommended vaccinations that have included vaccinations with pneumococcal conjugate vaccine (PCV) and Haemophilus influenzae type b conjugate vaccine (Hib) at 2 months, 4 months, and 6 months. What thoughts do you have about Billy?
The physician suspects that Billy has an immunodeficiency. Blood test results: Total WBC: 7,400/µl (4,100-10,900/µl) Differential WBCs: Neutrophils 55% (35-80%) Lymphocytes 35% (20-50%) Macrophages 8% (2-12%) Eosinophils 1% (0-7%) Basophils 1% (0-2%) All other blood test results are normal. What thoughts do you have about Billy? What additional tests might you wish to run?
Isotypes have different heavy chains. They are represent classes of antibody. Allotypes have the same constant regions with minor, but immunologic differences. Different individuals have different allotypes. Idiotypes are antibodies that recognize different specific epitopes. Each idiotype is composed of several idiotopes or combining sites.
Antibody Isotypes (Classes) Five major classes of antibody • IgM • IgD • IgG Subclasses: IgG1, IgG2, IgG3, IgG4 • IgE • IgA Subclasses: IgA1, IgA2
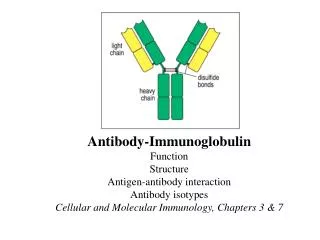
Structures of Different Isotypes (Classes) of Antibodies The different antibody isotypes (classes) differ in Number of subunits Number of domains, Number and location of carbohydrate chains, Presence or absence of hinge region, Number and location of disulfide bridges.
Concentrations of Serum Immunoglobulins Serum electrophoresis showing the mobility and relative amounts of the five classes of immunoglobulin. IgG is found in the region while most of IgM is found in the region.
IgM • Monomeric IgM is expressed on the surface of B cells where it serves the role of antigen recognition. • Pentameric IgM is expressed in the serum (5-10% of total serum Ab). • Pentameric IgM is secreted into mucosal secretions.
IgM Structure • The pentameric structure of IgM is stabilized by a J chain (joining chain) and by disulfide bonds. • Secretory IgM has a secretory component that assists in transport across the epithelial membrane. • Note that for IgM, the pentameric structure is shown as a flat molecule (like a hand flat on a surface). In reality, the disulfide bonds would all be the same length. In its binding form, the molecule would look more like a hand poised on a surface with only its fingertips touching the surface. This allows for multiple interactions with repeated epitopes on a given antigen.
Biological Functions of IgM • Good at virus neutralization • Poor at toxin neutralization • Excellent at bactericidal activity • Excellent at causing agglutination of antigens • Excellent at causing precipitation of antigens • Excellent at complement fixation • Does not bind to M Fc receptors • As a monomer, it serves as surface receptor for antigens on B cells
Medical Considerations of IgM • Elevated levels indicate a recent infection or other exposure to antigen • Does not cross placenta • Not useful for protecting immunocompromised individuals (short half-life and lower specificity than IgG) • Not useful as blocking antibody to block TNF production • Not useful as blocking antibody to block allergens • Not present in interstitial fluids (too big) • Can be present in bodily secretions
IgD • Monomeric IgD is expressed on the surface of B cells where it serves the role of antigen recognition. • IgD is a very minor component of serum Ig (0.2%) • Biological Functions: no biological effector function has been determined for IgD. • Medical Consideration: some multiple myeloma patients over-express IgD.
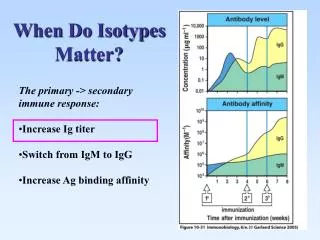
IgG • IgG is the predominant antibody synthesized during a secondary immune response (anamnestic response) • IgG is the most abundant class in serum, constituting 80% of serum Abs. • Although it cannot be transported across the epithelium, it is produced in the distal pulmonary tract and is important in pulmonary secretions. • There are four subclasses of IgG.
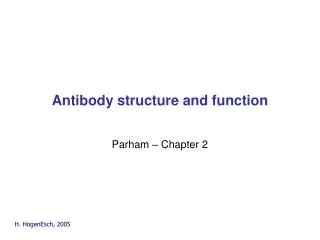
Four Subclasses of IgG Note the much longer Gamma chain on IgG3
IgG Subclasses Longer gamma chain
Biological Functions of IgG • Good at virus neutralization • Excellent at toxin neutralization • Good at bactericidal activity • Good at causing agglutination of antigens • Good at causing precipitation of antigens • Good at complement fixation • Binds to M Fc receptors
Medical Considerations of IgG • Crosses placenta providing protection to the fetus. • Can mediate hemolytic disease of the newborn (blue baby syndrome, Rh mismatch). • Can be used to protect immunocompromised (gamma globulin). • Can be used as blocking antibody to block TNF production (rheumatoid arthritis). • Can be used as blocking antibody to block allergens (desensitization to hypersensitivity) • Not present in most bodily secretions • Present in interstitial fluids
IgA • IgA is the predominant Ig in bodily secretions. • IgA in blood can be monomeric, dimeric, or trimeric. When multimeric, the J chain stabilizes the interactions of the two or three monomers. • IgA in bodily secretions is dimeric and combined with the J chain and with secretory component.
Secretion of IgA • Dimeric IgA molecules, stabilized as a dimer by the J chain is secreted into the blood by a plasma cell. • The dimeric IgA binds to the Poly-Ig receptor on the basolateral membrane of an epithelial cell. • The dimeric IgA, bound to the Poly-Ig receptor is internalized in an endocytic vesicle. • The Poly-Ig receptor is cleaved, with the larger peptide remaining associated with the dimeric IgA as secretory component. • The dimeric IgA, with secretory component, is released on the luminal side of the epithelial cell. • Secretory component protects IgA from enzymatic degradation.
Biological Functions of IgA • Excellent at virus neutralization • Excellent at toxin neutralization • Good at bactericidal activity • Good at causing agglutination of antigens • Good at causing precipitation of antigens • Does not bind to M Fc receptors
Medical Considerations of IgA • Daily production of IgA is greater than any other Ig. • B cells that will produce IgA migrate to subepithelial tissue of most mucosal epithelia and of glandular epithelia. • Present in bodily secretions. • Present at very high levels in colostrum and present in breast milk. Provides an excellent level of protection of newborns against respiratory and intestinal infections.
IgE • There is very little IgE in the blood (0.02% of Ig). • Most of the IgE is bound to Fc receptors on mast cells in the epithelial tissue and on basophils in the blood.
Biological Functions of IgE • Cross-linking of IgE molecules on the surface of a mast cell or basophil causes the release of histamine; the synthesis of prostaglandins, leukotrienes, and other chemokines; the production of various cytokines. • IgE plays a major role in combating parasitic infections. • IgE plays a role in combating pulmonary fungal infections.
IgE-Mediated Release of Histamine • The epitope of an antigen binds to an IgE paratope. • If another epitope of the antigen binds to the paratope of another IgE molecules, this causes cross-linking. • The cross-linking changes the character of the binding of the Fc receptors to the mast cell, initiating a trans-membrane signal. • The mast cell degranulates.
Medical Considerations of IgE • Individuals who express allergies to certain antigens over-produce IgE to those antigens. • This causes a high level of expression of IgE with the same paratopes (recognize same epitope on antigen) on given mast cells. This makes it easier to cross-link two IgE antibodies. • When antigen is present, many mast cells are degranulated, resulting in an over-stimulation of the immune system that is manifested as an allergic reaction (Type 1 hypersensitivity). • IgE plays an important role in asthma, too.
Events Associated With Mast Cell Degranulation
Billy Daniels Antibody levels in the blood: Serum IgG <1.0 mg/100 ml 350-800 mg/100 ml Serum IgA <1.0 mg/100 ml 15-50 mg/100 ml Serum IgM <1.0 mg/100 ml 25-75 mg/100 ml How do you interpret these results? What additional tests would you wish to run?
Billy Daniels Lymphocyte stimulation test: Phytohemaglutinin 136.2 134.3 Concanavalin A 47.9 48.8 Pokeweed mitogen 0.0 46.5 CD19* positive cells: undetectable How do you interpret these results? * A marker for B cells.
Billy Daniels Billy is diagnosed with X-linked agammaglobulinemia (Bruton’s agammaglobulinemia). This type of agammaglobulinemia is caused by a mutation in Bruton tyrosine kinase (Btk). Btk is needed for proliferation and differentiation of B cells. Btk mutatiions have variable severity from individual to individual, indicating that different mutations to Btk cause variable expressivity. He is given an intramuscular injection of IgG and will continue receiving these injections every 3-4 weeks for the rest of his life. In addition, Billy must be promptly given antibiotics any time he has a bacterial infection.