Download
1 / 34
360 likes | 692 Views
MRSA Screening. Bruce Gamage, RN BSN CIC Provincial Infection Control Network. Outline. Acute Care Rationale Cost/Benefit Screening Programs Notification/Flagging/Transfers Screening Health Care Workers Long Term Care Screening and Notification Admission Assessment/Room Placement

E N D
MRSA Screening Bruce Gamage, RN BSN CIC Provincial Infection Control Network
Outline • Acute Care • Rationale • Cost/Benefit • Screening Programs • Notification/Flagging/Transfers • Screening Health Care Workers • Long Term Care • Screening and Notification • Admission Assessment/Room Placement • Hemodialysis • Admission Screening • Prevalence Screening • Summary
Screening - Rationale • Undiagnosed MRSA colonization or infections in patients can contribute to the spread of AROs within a health care facility. • MRSA has become more common in healthy individuals living in the community, or in individuals with no prior admission to a hospital. • Without admission screening 84% of MRSA carriers would have been missed at admission and 76% during their hospital stay • Lucet, JC et al. ICHE; 2005; 26:121-26
Cost/Benefit of Screening Programs • The institution of routine nares swabs in all ICU patients (positive cultures resulted in contact precautions) over a 16 month period resulted in a 75% reduction in MRSA bacteremias in ICU patients (p=.007) and 40% in non-ICU patients (p=.008). • Huang SS et al. J Infect Dis. 2007 Feb 1;195(3):330-8.
Cost/Benefit of Screening Programs • At a cost of $3,475/month for the screening program averted 2.5 MRSA bacteremias/month for the ICU saving $19,714/month in excess costs • Clancy et al. ICHE; 2006: 27(10); 1009-1017
Screening Programs • All acute care hospitals should have a program of active surveillance for AROs for all admitted patients which includes: • screening/identification • followed by cultures if screening indicates.
Who should have screening cultures done? • Any patient with a previous admission to an acute care facility for a stay of from 12 to 48 hours during the last 3 to 12 months as determined by your facility and your health authority. • Patients who have been recently incarcerated, live in shelters, dormitories or other group settings. • Patients who have participated in contact sports or any sport activities using shared equipment. • Patients from long term care settings with known risk factors (examples: hemodialysis, chronic ventilation or skin breakdown). • Patients admitted from areas with higher endemic rates (examples: ICUs, Burn units, and Oncology units).
Should Previously Positive Patientsbe Screened? • Screening of previously positive patientsshould be made on a regional or local basis in consultation with laboratory. • Patients who are known to have tested positive for MRSA previously may be considered for repeat screening on a selective basis. • If not rescreened the patient should be considered MRSA positive.
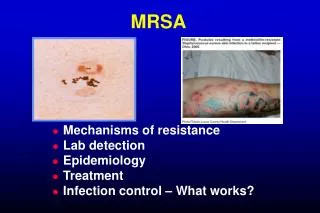
It is essential to culture all indicated sites • 16% of cases MRSA were culture positive only in the perianal area. • Williams V, Barry C, Verncombe M, Simor A: CJIC Spring 2005
Notification/Flagging • It is recommended that the patient’s medical record and/or computer file be flagged in some manner for future identification of MRSA status in order to facilitate prompt identification on readmission.
Transfers • The transferring facilities should inform receiving facilities of a patient’s colonization or infection history and MRSA • If a patient is deemed to have a new MRSA infection or colonization after being admitted from another institution, the receiving institution should inform the original institution of the patient’s status.
Discontinuing Precautions • The absence of MRSA/VRE on the surveillance swabs does not unequivocally mean that organism has been eradicated from the patient. • Discontinuing precautions on ‘swab negative’ patients must be made individually based on patient characteristics and institutional policies. • Many of these patients become colonized again when exposed to antibiotics, or if their condition worsens.
Screening Health Care Workers • Screening of HCW including Students physicians, and volunteers should be considered only if specific health care workers have been epidemiologically implicated in the transmission of MRSA.
Screening Health Care Workers • Identifying colonizedHCW through screening as part of an outbreak investigation should only be done at the direction of IPC and OHS, and in conjunction with the investigation of other possible sources of transmission. • Prior to proceeding with any HCW screening a discussion between OHS, IPC, diagnostic laboratories, and the MHO is recommended.
Routine pre-employment screening • Routine screening for MRSA of HCW carrying on activities in the hospital is not required
OHS Considerations Regarding MRSA • MRSA is not more likely to cause disease in healthy individuals than antibiotic susceptible organisms. • HCW are generally identified as asymptomatic carriers of MRSA • If acute illness develops, e.g. draining boils, the person should be managed according to current medical management recommendations and hospital policy specific to the illness.
Long Term Care Residential Care Facilities: Rehabilitation Facilities, Palliative Care, Complex Care, Psychiatric Care and Discharge Planning/Transition Units.
Admission • Admission should notbe denied or delayed by a LTCF on the basis of colonization or infection with an ARO. • All LTCFs should be prepared to implement the appropriate infection control measures and stringently follow Routine Practices for persons who are colonized or infected with an ARO
Screening and Notification • Routine screening for MRSA is not currently recommended for residents/ clients of LTCFs in BC. • Each facility should base decisions regarding admission screening for AROs by assessing each resident for the presence or absence of risk factors.
Admission Assessment • An assessment of factors related to risk of colonization or infection with MRSA or other AROs is considered part of the long term care resident’s general admission assessment. • Each facility should base decisions regarding MRSA screening cultures, room placement and use of additional precautions on the results of this risk assessment.
Room Placement based on Risk Assessment • If possible, patient or resident placement decisions should be made before the patient or resident arrives. • Room placement for residents/clients with AROs should take into consideration: • cognition, compliance, continence, and degree and site of colonization for all individuals in the room. • Placement options include either a single room or: • sharing a multi-bed room with other patients or residents/clients also with the same or other AROs (cohorting), • sharing a multi-bed room with other persons not colonized. • Infection Control should be consulted regarding specific placement questions as required.
Admission Screening • Admission to any hemodialysis unit should not be denied to any BC resident on the basis of ARO status.
Screening Indications: Admission Screening for MRSA/VRE will be completed when the patient is first received on the hemodialysis unit: • On initial admission to a Community Hemodialysis Unit (CDU), In-center Hemodialysis Unit (HD) or Peritoneal Dialysis Unit (PDU) • Upon return from admission to an acute care hospital or a care facility • Upon returning from travel • All Peritoneal dialysis patients after temporary hemodialysis unless swabbed within the previous two weeks
Screening Indications: LTC Long-term Care Patients Receiving Hemodialysis: • On admission to an acute care facility from residential care • During hemodialysis prevalence screening • As clinically indicated
Screening Indications: Visitors and Travelers Incoming Visiting Patients or (Travelers) • The decision to accept visitors for dialysis will be based on receiving a current ARO status report before the patient arrives. • Screen all visiting HD patients upon arrival. • Patients returning from travel inside Canada are screened but not isolated • Patients returning from travel outside Canada are screened, isolated in a private room/separate area on Contact isolation Outgoing Traveling Patients • Patients who will be traveling out of BC may be requested to demonstrate current ARO status. • Results of ARO screen are included with the patient’s clinical information and forwarded to the receiving dialysis unit.
Prevalence Screening • The decision, frequency, sites screened and AROs screened for are based on the specific facility and program’s unique indicators, epidemiology, resources and capacity for prevalence screens.
Screening Indications: MRSA or VRE Positive • Patients with a laboratory-confirmed ARO are not routinely screened for the known/alerted ARO. • Patients who are MRSA positive will be screened for VRE. • Patients who are VRE positive will be screened for MRSA.
Summary • Acute Care • Rationale/Cost-Benefit of Screening Programs • Screening Health Care Workers • Long Term Care • Screening and Notification • Admission Assessment/Room Placement • Hemodialysis • Admission Screening • Prevalence Screening
Questions? • bgamage@phsa.ca • 604-660-6076