Download
1 / 26
260 likes | 431 Views
Atherosclerosis Infarction. Atherosclerosis. Atherosclerosis is a specific form of arteriosclerosis (thickening & hardening of arterial walls) affecting primarily the intima of large and medium-sized muscular arteries and is characterized by the presence of fibrofatty plaques or atheromas.

E N D
Atherosclerosis • Atherosclerosis is a specific form of arteriosclerosis (thickening & hardening of arterial walls) affecting primarily the intima of large and medium-sized muscular arteries and is characterized by the presence of fibrofatty plaques or atheromas. • The term atherosclerosis is derived from athero (meaning porridge) referring to the soft lipid-rich material in the centre of atheroma, and sclerosis (scarring) referring to connective tissue in the plaques.
Atherosclerosis • Most commonly affected arteries by atherosclerosis include large and medium sized arteries like aorta, coronary, popliteal and cerebral arteries. • Major complications resulting from ischemia due to atherosclerosis include myocardial infarction leading to heart attacks and cerebral infarction leading to strokes. • Less common complications include peripheral vascular disease, aneurysmal dilatation due to weakened arterial wall, chronic ischemic heart disease, ischaemic encephalopathy and mesenteric occlusion.
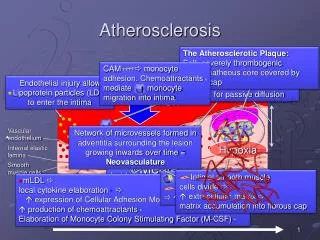
Concepts of atherogenesis Hyperlipideamia, Hypertension, Smoking, Homocysteine, Hemodynamic factors, etc Endothelial Injury/Dysfunction Endothelium(E) Subendothelial space Smooth muscle layer(S) Adventitia
Concepts of atherogenesis Circulating platelets adhere to endothelial surface Leukocyte adhesion Leukocyte migration Taken from Robbins Pathologic Basis of Disease
Concepts of atherogenesis Endothelial Permeability increased LDL, VLDL and leukocyte accumulation Smooth muscle migration
Concepts of atherogenesis Gross appearance of fatty streaking Macrophage and smooth muscles engulfing more and more LDL Arrival of lymphocyte
Risk Factors in Atherosclerosis Major risk factors 1) Major Constitutional risk factors: i. Age ii. Sex iii. Genetic factors iv. Familial and racial factors 2) Major Acquired risk factors: i. Hyperlipidaemia ii. Hypertension iii. Diabetes mellitus iv. Smoking v. Hyperhomocysteinemia
Risk Factors in Atherosclerosis Minor Risk Factors: 1. Environmental influences 2. Obesity 3. Hormones: Oestrogen deficiency, oral contracep. 4. Physical inactivity 5. Stressful life 6. Infections (C. pneumoniae, Herpes virus, CMV) 7. Homocystinuria 8. Role of Alcohol
Progression of Atherosclerosis • Endothelial Injury: • include mechanical trauma, haemodynamic forces, immunological and chemical mechanisms, metabolic agents like chronic hyperlipidaemia, homocystine, circulating toxins from systemic infections, viruses, hypoxia, radiation, carbon monoxide and tobacco products. • In humans, two major risk factors are haemodynamic stress from hypertension and chronic hyperlipidaemia.
Progression of Atherosclerosis • Intimal Smooth Muscle Cell Proliferation • Endothelial injury causes adherence aggregation and platelet release reaction at the site of exposed subendothelial connective tissue. • Proliferation of intimal smooth muscle cells is stimulated by various mitogens released from platelets adherent at the site of endothelial injury. • These mitogens include PDGF, fibroblast growth factor, TGF-ά. • Proliferation is also facilitated by nitric oxide and endothelin released from endothelial cells.
Progression of Atherosclerosis 3. Role of Blood Monocytes • Though blood monocytes do not possess receptors for normal LDL, LDL does appear in the monocyte cytoplasm to form foam cell. • Plasma LDL on entry into the intima undergoes oxidation. Oxidised LDL formed in the intima performs following two important functions : • For monocytes, oxidized LDL acts to attract, proliferate, immobilise and activate them and is readily taken up by scavenger receptor on the monocyte to transform it to a lipid laden foam cell. • For endothelin, oxidized LDL is cytotoxic.
Progression of Atherosclerosis 4. Role of Hyperlipidaemia • Chronic hyperlipdaemia in itself may initiate endothelial injury and dysfunction by causing increased permeability. • Increased serum concentration of LDL and VLDL promotes formation of foam cells, while high serum concentration of HDL has anti-atherogenic effect.
Progression of Atherosclerosis 5. Thrombosis • Endothelial injury exposes sub-endothelial connective tissue resulting in platelet aggregation at the site besides proliferation of smooth muscle cells. • This causes mild inflammatory reaction which together with foam cells is incorporated into atheromatous plaque. • Lesions enlarge by attaching fibrin and blood cells causing thrombus formation which becomes a part of atheromatous plaque.
Infarction • Ischemic necrosis caused by occlusion of arterial or venous vessles. • Example: MI, cerebral infarction, pulmonary infarct, bowel infract, gangrene • 99% due to thrombosis, mostly arterial • Can be: • Vasospasm • External pressure • Trauma • Twisting of organs eg. Testicular torsion • Edema
Venous infarct occurs in organs with single venous outflow. Eg. Testis, ovary • Types: Red infarct, white infarct, septic infarct • Red infarct: • Due to venous occlusion • In loose tissue eg. Lung • Organs with dual circulation • In tissues that have be previously congested • White infarct • Arterial occlusion of solid organs, eg. Heart, kidneys, spleen
Infarction is usually wedge shape surrounded by rim of hyperemia • Hemosiderin pigment may accumulate following hemorrhage • Necrosis is of coagulative type (except brain: liquifactive) • Inflammation within few hours • Repair process
Factors influencing development of Infarct • Nature of the blood supply • Dual: lung, liver, hands • End-arterial: spleen, kidneys • Rate of occlusion: • Eg. Atherosclerosis of coronary arteries is gradual slow process
3. Vulnerability to hypoxia • Neuron: 3-4 minutes • Heart: 20-30 minutes • Fibrous tissue: hours 4. Oxygen content of the blood • Eg. Heart failure patient have low oxygen concentration in blood
Determinants of infarct outcome • Nature of vascular supply • Dual blood supply or collateral vessels • Rate of development of occlusion • Slowly occluded vessels become organized with alternate perfusion pathways of collateral circulation • Vulnerability to hypoxia • Neurons, 3 – 4 minutes • Myocardial cells, 20 – 30 minutes • Fibroblasts, skeletal muscle, hours • Blood oxygenation • Anemia or cyanosis exacerbates hypoxia
Ischemic coagulative necrosis • Histological changes appear in 4 to 12 hours after anoxia • Cellular swelling, membrane degradation, nuclear condensation and breakdown • Inflammation is well defined in 1 to 2 days • Reparation follows • Labile tissues regenerate • Stable tissues scar