Download
1 / 19
190 likes | 358 Views
Slides presented by the FDA at the Endocrinologic & Metabolic Drugs Advisory Committee meeting on June 10, 2003. Use of GH in idiopathic short stature. Efficacy for final height Guyda Survey 1999 (N= 413) Lilly GDCH (N=25) Lilly E001 (N= 50)

E N D
Slides presented by the FDA at the Endocrinologic & Metabolic Drugs Advisory Committee meeting on June 10, 2003
Use of GH in idiopathic short stature • Efficacy for final height • Guyda Survey 1999 (N= 413) • Lilly GDCH (N=25) • Lilly E001 (N= 50) • Finkelstein meta-analysis (84 GH –104 C) • Cost benefit analysis • Bailey 1992 • Bryant 2002 • Ethics • Psychosocial enhancement • Fairness, social policy, resource allocation
Definition of Idiopathic Short Stature • Normal size at birth (> - 2 SDS) • Significant short stature (< -2 SDS) • The tempo of growth may be slow or normal • No evidence of: • Systemic disease • Malnutrition • Hypothyroidism • GHD From: Ranke MB, Towards a consensus on the definition of idiopathic short stature. Horm Res 45:64-66, 1996
Spontaneous Adult Height in Patients with Idiopathic Short Stature.Price: Horm Res 45:59, 1996 Study (N) Males Females HT/FAH SDSHT/FAH SDS Ranke (25) 1982 -2.1/-1.1 -2.7/-2.4 Volta (41) 1988 -1.7/-0.9 -1.7/-0.8 Brams. (69) 1990 -2.2/-0.7 -2.1/-0.7 Crowne (58) 1991 -3.4/-1.6 -3.4/-1.5 LaFran. (42) 1991 -2.0/-1.2 -2.0/-1.3 Ranke (236) 1995-2.0/-0.8-2.0/-0.8 Mean (471)-2.2/-1.0-2.3/-1.1 Adult height gain + 1.2 + 1.2
Comments on GDCH Study • Enrollment errors: baseline height velocity was calculated for only six months prior to randomization, subjects included SGA children, older age group with BA of 13 in boys 11 in girls, with Tanner 2 puberty in some, and patients with hypothyroidism treated for only 3m. • Therapeutic regimen was inadequate as the dose was low for children with normal GH secretion, and given only 3x weekly. This issue was noted at the FDA meeting in 1987 . • High drop out rate: only 16 GH (42%) and 9 placebo (27%) completed the study. Possible bias of positive benefit. • The overall treatment effect was very modest: Mean final height gain of + 0.51 SDS or + 3.7 cm. This would move a boy from –2.25 SDS (1.2 % ile) to –1.88 SDS (3rd % ile). • He would still be 12 cm below the mean. • GDCH psychological data was not provided to FDA.
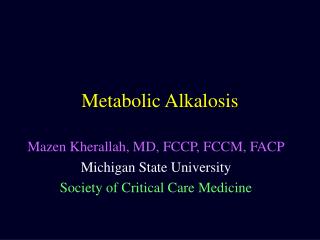
<=66 >66 72 68 64 Last Height (inches) Females 60 56 52 48 N= 4 N= 2 72 68 64 Last Height (inches) Males 60 56 52 48 N= 13 N= 5 N= 5 N= 3 HUM PLA HUM PLA
Dose effect from + 0.33 SDS to + 1.29 SDS and +2.3 to + 7.3 cm. Significant numbers overlap GDCH placebo group (Figure 18, Page 32). High drop out rate: 30/239 (12.6%) in first two Years, and only 50 left in final height cohort (21% of randomized subjects), with almost half being at one Dutch center. The highest drop out for patient request (38 or 46%) was in the high GH dose group – why if clinical “benefit” was most positive in this group? Comments on Study E001
Finkelstein et al. Effect of GH therapy in children with ISS: A Meta Analysis. • Dr. F. Ducharme, Pediatric Editor of Cochrane reviews rated this meta analysis as Level 2 – a mixture of controlled and uncontrolled or non randomized studies, with small numbers, hence a likely bias to positivity. (Level 1 best). • Only 4 controlled studies (CCT) to adult height: 84 GH and 104 C. Multiple dropouts reported. • Gain observed was + 0.54 SDS (3.6 – 4.6 cm) over predicted, and + 0.84 SDS (5-6 cm) over control group. True estimates by RCT are likely to be smaller than by CCT. • NB: < 10th percentile used, and SGA included.
ECONOMIC PERSPECTIVES IN USA:Bailey A: Growth, Genetics, Hormones 1992 • Defense $303.6 billion • Alcohol $ 25.6 billion • Tobacco $ 23.6 billion • Medicaid (6-20 yr.) $ 6.2 billion • N.I.H. $ 6.8 billion • Lowest 1% height $ 3.0 billion
Study category Sex Untreated adult height (cm) GH dose (mg/kg/w) GH adult height (cm) Cost /cm (USD) Normal M 178 - - - F 164 - - - GHD M 134-146 .18-.35 168 10,000 F 128-134 .18-.35 155 10,000 CRF M 156 .30-.35 162-165 11-38,000 F 152 .30-.35 151-155 11-38,000 ISS M 150-170 .20-.40 164 22-43,000 F 137-156 .20-.40 155 25-43,000 TS F 143 .375 146 25-28,000 Cost effectiveness of adult height gain with GH treatment Constructed from data by Bryant et al., Health Technol Assess 2002:Vol 6, No 18, 1-168
When is being short a medical problem? • “Short stature” is not a medical diagnosis. It is a descriptive term for a person whose height is considered significantly below the normal range of measurements for that age, gender, racial group or family. • Short stature is also a statistical term, generally referring to people who are shorter than 97% of their age and sex matched peers. Thus, in any population, nearly 3 out of each 100 persons will meet this statistical definition, most with no discernable medical abnormality. • Height perception is influenced by a wide variety of factors: culture, gender, family background, and psychological state.
Is short stature a psychological burden requiring GH therapy? • Sandburg 1994: Short stature does not appear to be associated with clinically significant psychosocial morbidity. • Gilmore & Skuse 1996, 1997: Little evidence was found to suggest clinic referred untreated prepubertal short children are psychologically maladjusted. • Downie et al 1996: To date, no psychological benefits of GH treatment have been demonstrated. • Zimet et al 1997: Adults evaluated for SS but not treated with GH as children do not show psychosocial distress or impairment and does not provide a basis for GH treatment of ISS.
Equipoise & Benefit Assignment Equipoise demands that the following three psychological effects are considered before assigning benefit in short children treated with Growth Hormone: • Beneficial - with improved self-esteem due to increased height velocity or increased final adult height (FAH). • Harmful- due to disappointment with FAH or poorer self-esteem due to increased medicalization, daily GH injections, etc. • Neutral – no psychological benefit.
The Use of Growth Hormone in ISS Summary and Conclusions I: • The number of subjects in randomized controlled studies of GH therapy to FH is very limited, including GDCH. • FH gain in GDCH was + 0.51 SDS or + 3.7 cm. Treated data points show considerable overlap with placebo group – is this clinically significant? • The majority of studies are uncontrolled, and final adult height attainment over predicted adult height has averaged < 1.0 SDS. • This is identical to the spontaneous height gain in children with idiopathic short stature.
Summary and Conclusions II: • In one study of 236 normal short children (Ranke 1995), 67% spontaneously achieved normal adult height, 23% did not, and only 10% did not reach familial target height. • Few studies address the downside or negative outcome; in Australia (Cowell 1996), 464 children out of 1362 (34%) who commenced GH therapy for short stature did not complete 3 years of therapy. • In GDCH only 28% placebo and 42% GH therapy subjects completed the study. • Few studies have addressed the psychological benefit of GH treatment to final height for idiopathic short stature. This remains unproven.
Bryant J. Cave C. Mihaylova B. Chase D. McIntyre L. Gerard K. Milne R. Clinical effectiveness and cost-effectiveness of growth hormone in children: a systematic review and economic evaluation. [Review] [105 refs] [Journal Article. Review. Review, Academic] Health Technology Assessment (Winchester, England). 6(18):1-168, 2002.




![STN 125011 Tositumomab Therapeutic Regimen (TTR) [tositumomab plus I-131 tositumomab]](https://cdn2.slideserve.com/4678696/stn-125011-tositumomab-therapeutic-regimen-ttr-tositumomab-plus-i-131-tositumomab-dt.jpg)
