Download
1 / 36
360 likes | 460 Views
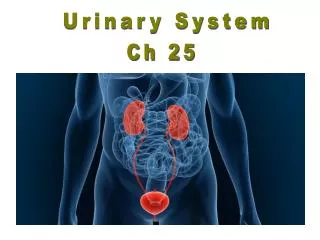
Urinary System. I. Introduction . A. Organs/Structure Kidneys Ureter Urinary Bladder Urethra. Introduction. Function Removes waste material from blood Primary organ responsible for monitoring blood composition. II. Kidneys. Function

E N D
I. Introduction A. Organs/Structure • Kidneys • Ureter • Urinary Bladder • Urethra
Introduction • Function • Removes waste material from blood • Primary organ responsible for monitoring blood composition
II. Kidneys • Function • Maintain homeostasis by regulating blood composition (water, electrolytes), pH, & blood volume • Secrete hormone erythropoietin to control rate of RBC production • Vitamin D activation • Renin – secreted to maintain blood volume and pressure
Kidneys • Anatomy • Shape & size: bean-shaped; 4-5 oz, 4”x3”x1” enclosed in tough fibrous capsule • Location • Retroperitoneal – between T12 & L3 • Left is slightly higher, surrounded by fat for protection • Cortex • Outer margin • Dips into medulla between pyramids, creating renal columns
Kidneys 4. Medulla a) inner portion b) Divided into 12 -18 triangular structures Pyramids c) Pyramids have striated appearance 5. Hilus a) medial, concave depression b) site where renal blood vessels enter/leave the kidney and where ureter exits
Kidney 6. Renal Pelvis a) funnel-shaped expansion of upper ureter that collects urine b) major/minor calyces – divisions of renal pelvis
Kidney 7. Nephron - Cortex a) functional unit: ≈ 1 million/ kidney b) Renal corpuscle • Glomerulus – cluster/ball of capillaries • Bowman’s capsule – thin-walled expansion of proximal tubule that forms a cup over the glomerulus
Kidney C) Renal tubules • Proximal convoluted tubule: in cortex, highly coiled • Descending and ascending: Loop on Henle; found in medulla • Distal convoluted tubule: cortex; highly coiled • Collecting tubule: collects and delivers urine to calyx
Kidneys d) Renal Arteries: arteriole capillariesarteriole • Afferent arteriole brings blood to glomerulus • Blood is filtered no loss of O2 • Efferent Arteriole: blood (minus filtered fluid) exiting glomerulus • Smaller diameter than efferent • Causes blood to back-up in the glomerulus which ↑ filtration rate • Peritubular Capillary • Efferent arteriole branches into capillaries which surround renal tubule • Juxtaglomerular apparatus • Associated with afferent and efferent arterioles • Controls renin secretion in order to control blood volume and blood pressure
III. Urine Formation • Glomerular Filtration 180 L/ 24 hours • Passive, non-selective process • Movement of water + dissolved substances from capillaries to Bowman’s capsule • Similar to tissue fluid • Glomerular Filtration Rate • Volume of filtrate formed each minute • Factors • Total surface area available for filtration • Filtration membrane permeability • Net Filtration Pressure (NFP) a) Hydrostatic pressure created by afferent and efferent arteriole sizes
Urine Formation 5. Regulation of GFR: need to maintain fairly constant GFR a) Intrinsic controls • Renal autoregulation • Adjustment of resistance to blood flow (vasoconstrict or vasodilate afferent arteriole) b) Extrinsic controls • sympathetic nervous system controls • During stress, when it is necessary to shunt blood to important organs, neural controls overcome autoregulation • Afferent arterioles (i) Norepinephrine constricts afferent arteriole = ↓ filtrate formation
Urine Formation 2. Renin – released by juxtaglomerular cells a) Renin angiotensis II b) Angiotensin II potent vasoconstrictor of smooth muscle in arteriole wall = ↑BP c) stabilizes systemic BP d) partially restores glomerular filtration rate to normal levels
Urine Formation 3. AtrialNatriuretic Peptides (ANP) a) secreted by heart b) ↑Na+ excretion, ↑glomerular filtration rate, ↓water reabsorption = ↑urine output
Urine Formation • Tubular Reabsorption Back to Blood • Filtered substances • Proximal convoluted tubule • Most reabsorption • Glucose reabsorbed via active transport • Sodium • Sodium pump (active transport) moves Na+ • Various negatively charged ions follow • Water • Follows • Osmosis (passive) water movement • Water can leave descending loop of Henle
Urine Formation C. Tubular Secretion Blood to Nephron • Substances move from peritubular capillaries • H+, NH3, K+
Urine Formation • Aldosterone • Adrenal gland • Released due to changes in blood concentrations of Na+ & K+ • Distal convoluted tubule stimulated to reabsorb (by blood) Na+ & secrete K+ (into urine) • ↑ water reabsorption by blood leads to ↓ urine output
Urine Formation 2. Antidiuretic Hormone (ADH) a) hypothalamus produces - posterior pituitary releases b) released in response to ↓ blood water levels c) distal convoluted tubule wall permeability changes and water is reabsorbed by peritubular capillaries d) urine volume ↓
Urine Formation E. Composition • Urea • by-product of amino acid catabolism • 50% reabsorbed; rest in urine • Uric Acid • by-product of metabolism of organic bases in nucleic acids • Little is excreted • ↑ uric acid in gout
Urine Formation 3. Composition varies with diet 4. Volume a) between 0.6 – 2.5 L/day b) due to intake, environmental temp., body temp., humidity, respiratory rate
V. Ureters ≈ 25 cm long • Carry urine from pelvis to bladder • Anatomy • Mucosa • Muscularis – 2 smooth muscle sheets longitudinal & circular • Adventitia – connective tissue outer layer
Ureters C. Function: Plays active role in transporting urine through muscle contractions D. Homeostatic Imbalance • Renal caculi = kidney stones • Size – most <5mm & pass without problems • Pain – larger caculi may obstruct ureter, causing ↑ pressure in kidney excruciating pain
Ureters C. Predisposing conditions • Frequent bacterial infections • Urinary retention • High levels of blood calcium • Alkaline urine D. Treatment • Shock wave lithotripsy • Acidification of urine drink cranberry juice
V. Bladder • Muscle sac that receives and stores urine • Collapsible • Male – prostate surrounds bladder neck • Anatomy • Trigone • Smooth triangular region in base of bladder (not muscular) • Outlined formed by openings for both ureters and the urethra • Infections tend to persist in this region
Bladder 2. Bladder wall • Mucosa – contains transitional epithelium • Muscular layer • Inner and outer longitudinal muscles • Middle circular layer • Fibrous adventitia – outer connective tissue covering 3. Rugae – folds that occur when empty bladder collapses
Bladder C. Function • Stores urine temporarily • Holds ≈ 500 mL; Max: 800 – 1000 mL
VI. Urethra • Canal for excretion of urine from body • Anatomy – thin-walled muscular tube • Female: 1.5 in. long • Male: 8 in long; double function – carries both urine & semen
Urethra C. Internal urethral sphincter – Involuntary • At bladder/urethral junction (smooth muscle) • Contraction opens sphincter; relaxation closes it • Prevents leaking between voiding D. External urethral sphincter • Voluntary • Formed by skeletal muscle
Urethra E. Homeostatic Imbalance – Urinary Tract Infection • Improper toilet habits: female opening is close to anus • Sexual activity • Intercourse drives bacteria into vagina and external genital region toward bladder • Spermacide magnifies problem because it kills helpful bacteria, allowing infectious fecal bacteria to colonize vagina • 40% of all women get UTI’s • Urethral mucusa is continuous with bladder, uretal, kidney mucosa a) Inflammation of urethra (urethritis) can ascend the tract cystitis pyelonephritis
Urethra 4. Symptoms • Dysuria – painful urination • Urgency & frequency • Fever • Cloudy or blood-tinged urine • Sever headache, backache, lower abdominal ache
VII. Congenital Abnormalities • Horseshoe Kidney – 1 out of 600 births • Kidneys fuse across the midline, forming single, u-shaped kidney • Usually asymptomatic; may be assoc, with other abnormalities of kidney
Congenital Abnormalities B. Hypospadias – males only • Most common congenital abnormality of urethra • Urethral orifice located on ventral side of penis (corrected surgically ≈ 1 yr)
Congenital Abnormalities C. Polycystic Kidney Disease (PKD) – Group disorders • Fluid-filled cysts – interfere with renal function, leading to renal failure • Less severe form – 1 in 500 a) inherited in autosomal dominant fashion b) cysts develop gradually, no symptoms until 40 c) by 60’s, kidneys become knobby and enlarged, up to 30 lbs each
Congenital Abnormalities • More severe form – less common • Autosomal recessive inheritance • ≈ ½ of newborns with recessive PKD die just after birth, survivors develop renal failure in early childhood • Results from mutation in single gene • Treatment • Renal dialysis • Kidney transplant
VIII. Aging • Kidneys • Only 3% of elderly have histologically normal kidneys • Kidney function↓ with age • Kidneys shrink as nephrons decrease in size and # • By age 80, GFR is ½ that of middle-aged adults • Diabetics are particularly at risk
Aging • Bladder • Shrunken, with < ½ capacity of a young adult • Loss of bladder tone causes an increase in urination frequency • Nocturia (excessive urination at night) plagues 2/3’s of this group • Many eventually experience incontinence