Download
1 / 30
300 likes | 429 Views
Masterclass - Coronary Heart Disease Competitor analysis correct at time of publishing. July 2014. For advisers only. Agenda. The role of the heart Anatomy of a heart attack How critical illness defines a heart attack How PruProtect defines a heart attack Underwriting considerations

E N D
Masterclass - Coronary Heart DiseaseCompetitor analysis correct at time of publishing July 2014 For advisers only
Agenda • The role of the heart • Anatomy of a heart attack • How critical illness defines a heart attack • How PruProtect defines a heart attack • Underwriting considerations • PruProtect - unrivalled cover for conditions affecting the cardiovascular system
The heart • A normal heart beats 100,000times a day or 3 billiontimes in an average lifetime • Each day it pumps 5,000 gallonsof life sustaining blood through a60,000mile network of vessels • Blood takes approximately 20 secondsto circulate throughout the entire vascular system Source: https://www.bhf.org.uk/heart-health/how-your-heart-works.aspx 2014
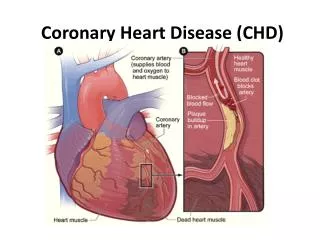
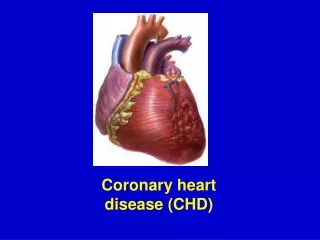
Anatomy of a Heart Attack? A coronary artery becomes narrowed It cannot deliver enough oxygen-containing blood to the heart muscle The inside lining of the narrowed artery cracks, a blood clot may form over the cracks This makes the artery even narrower and can quickly block off the artery If the artery is blocked for more than a few minutes, the muscle cells in the heart may become permanently damaged Often, the amount of muscle damage is small and, once the heart attack is over, there is enough good muscle left for the heart to carry on its work satisfactorily
Accounting for over a third of deaths, cardiovascular disease (CVD) is by far the biggest killer Just under 50% of deathsdue to CVD are from coronary heart disease CVD is one of the main causes of premature death, accounting for 30% of premature deaths in men and 22% of premature deaths in women Impact of cardiovascular disease Death by cause in men under 75, UK 2010 Source: http://www.bhf.org.uk/plugins/PublicationsSearchResults/DownloadFile.aspx?docid=508b8b91- 1301-4ad7-bc7e-7f413877548b&version=-1&title=Coronary+Heart+Disease+Statistics+2012+&resource=G608- 2012
Medical and demographic trends How heart disease has changed Over 17,000% increase in life saving prescriptions since CIC was launched Heart disease death rates halved since 1961 Source: http://www.bhf.org.uk/plugins/PublicationsSearchResults/DownloadFile.aspx?docid=508b8b91- 1301-4ad7-bc7e-7f413877548b&version=-1&title=Coronary+Heart+Disease+Statistics+2012+&resource=G608 - 2012
Preventing and treating a heart attack Angioplasty Angioplasty can help to relieve angina symptoms and is also used as an emergency treatment for people who've had a heart attack
Angioplasty key facts The importance of our unique definition Most angioplasty’s are performed on a single vessel Most people who undergo angioplasty haven’t suffered a heart attack c 5 x the number of Angioplasty to CABG Angioplasty (Coronary) or PTCA (Percutaneous Transluminal Coronary Angioplasty) – Severity F PTCA or other percutaneous coronary artery procedures performed by a Consultant Cardiologist to dilate and treat a coronary artery stenosis. The procedure may or may not involve the use of a stent Dr Rod Stables, The Cardiothoracic Centre, accessed 2014
ABI definition Pre 2006 Heart attack The death of a portion of heart muscle, due to inadequate blood supply, that has resulted in all of the following evidence of acute myocardial infarction: • typical chest pain; • new characteristic electrocardiographic changes; • the characteristic rise of cardiac enzymes, troponins or other biochemical markers; where all of the above shows a definite acute myocardial infarction Other acute coronary syndromes, including but not limited to angina, are not covered under this definition
Industry definition Heart Attack of specified severity • Death of heart muscle, due to inadequate blood supply, that has resulted in the following evidence of acute myocardial infarction: • Typical clinical symptoms (for example, characteristic chest pain) • New characteristic electrocardiographic changes • The characteristic rise in cardiac enzymes or troponins recorded at the following levels or higher; • Troponin T>1.0ng/ml • Accu Tnl > 0.5ng/ml or equivalent threshold with other Troponin I methods • The evidence must show a definite acute myocardial infarction • For the above definition, the following are not covered: • Other acute coronary syndromes including but not limited to angina
Typical clinical symptoms Not every person suffering a heart attack will have obvious symptoms • The symptoms of a heart attack vary from one person to another • They may feel tightness or pain in the chest • For some people, the pain or tightness is severe • Others may feel nothing more than a mild discomfort • They may feel • light-headed or dizzy • short of breath • nauseous • vomiting
New characteristic ECG changes “not all heart attacks can be detected by ECG” Source: http://www.patient.co.uk/health/electrocardiogram-ecg | http://www.thrombosisadviser.com/en/acs/a-leading-cause-of-mortality/ - 2014
Characteristic rise on cardiac enzymes/troponins • The current ABI levels were set in 2006 • Since then troponin assays have become significantly more sensitive , with some now measuring as little as a few picograms (a picogram being 1/1000th of a nanogram [ng]). • Currentclinical practice suggests a troponin T level of 0.1ng/ml or less as the criteria for diagnosis of a probable MI, well below the current ABI level of 1ng/ml
Our definition Heart Attack of specified severity Death of heart muscle, due to inadequate blood supply, that has resulted in the following evidence of acute myocardial infarction: • New characteristic electrocardiographic changes, and • The characteristic rise of cardiac enzymes or Troponins recorded at the following levels or higher; • Troponin T > 0.5 ng/ml • AccuTnI > 0.5 ng/ml or equivalent threshold with other Troponin I methods The evidence must show a definite acute myocardial infarction For the above definition, the following are not covered: • Other acute coronary syndromes including but not limited to angina Payable at severity C – 50% to a maximum of £1,500,000 We will now pay more heart attack claims
Our unique definition Heart Attack Death of heart muscle, due to inadequate blood supply that has resulted in the following: Definite Diagnosis of an acute Myocardial Infarction by a consultant cardiologist, which is supported by current medical reports, tests and investigations, as defined by the recognised international standard* prevailing at the time of claim For the above definition, the following are not covered: • Other acute coronary syndromes including but not limited to unstable angina. • Myocardial Infarctions that meet the international standard that occurred before cover commenced *(International standard defined by the European Society of Cardiology or the universal standard definition of Myocardial Infarction) Payable at severity D – 25% to a maximum of £750,000 We will now pay ALL heart attack claims
Competitor overview Highlighting PruProtect’s unique cover for heart attack Source: PruProtect Analysis
Why PruProtect for Heart Attack • We will pay 25% on diagnosis of ALL art attacks • We do not require characteristic ECG changes
Heart attack What this all means The Need What are we doing? Covering diagnosis of All heart attacks Traditional cover requires a heart attack to be a specified severity It’s the UK’s biggest killer 45% More likely to payout compared to industry standard definitions Most consumers expect a heart attack to be covered no matter how severe We now cover ALL heart attacks
Underwriting considerations Risk factors of CHD • Smoking • High blood pressure • High blood cholesterol • Diabetes -Decline • Being physically inactive • Being overweight or obese • Family history of heart disease • Ethnic background • Gender - men are more likely to develop CHD at an earlier age than women. • Age - the older you are, the more likely you are to develop CHD. • It is more acceptable for an older person to have a heart attack than a younger person and our ratings reflect this: • A 46 year old with heart attack +- 200% • A 66 year old with heart attack +- 125%
Underwriting considerations What does the underwriter need before making a decision? • TGPR to include sight of all investigations and surgical procedures • Date of onset and date of most recent symptoms • Has there been more than one heart attack (increase rating if 2, but decline if more) • Other risk factors present (as previously mentioned) Better risk • Older age, N/S, BP and Lipids all normal, single event, normal BMI, healthy lifestyle Poorer risk • Younger age, smoking, obese, more than one event, questionable lifestyle Definite declines • Combination of CHD and diabetes, client < age 40, >30 cigs pd, > 2 heart attacks
Underwriting considerations Some case studies • 44 year old male-angina first diagnosed 8 months ago, now stable. No surgery pending Postpone for 4 months then will require TGPR 2. 65 year old female. Heart attack in 2010 with single vessel bypass at the time. Has been well since but still smoking 10 cigarattes per day A loading in the region of 50-100% will be applied 3. 55 year old male. Had a heart attack in 2009 and then another in 2011 followed by a 2 vessel stent and has been well since A loading of 200-250% will be applied 4. 32 year old with a poor FH of CAD and who has had been suffering from angina since age 31. Maybe going in for an angiogram in next few months Decline
PruProtect - unrivalled cover for conditions affecting the cardiovascular system
Tools for you Article Email Cover magazine