Download
1 / 24
250 likes | 877 Views
Aortic Aneurysms. Mark A. Farber, MD. Aortic Aneurysms Incidence. 30-60/1000 Increasing incidence over past 3 decades Incidence of AAA Autopsy 1.5-3.0% U/S Screening 3.2% Pts with CAD 5.0% Pts with PVD 10.0% Pts with femoral and pop.aneurysms 50.0%.

E N D
Aortic Aneurysms Mark A. Farber, MD
Aortic AneurysmsIncidence • 30-60/1000 • Increasing incidence over past 3 decades Incidence of AAA Autopsy 1.5-3.0% U/S Screening 3.2% Pts with CAD 5.0% Pts with PVD 10.0% Pts with femoral and pop.aneurysms 50.0%
Aortic AneurysmsDefinition • Pseudoaneurysm • True Aneurysm
Definitions • Aneurysm - Increase in diameter of 50% (1.5x) its normal diameter – Focal region • Ectasia - Diffuse dilatation of an artery with increase in diameter >50% • Arteriomegaly - Diffuse enlargement of an artery, but not lg. Enough to meet criteria for an aneurysm
Aortic AneurysmsAssociated Aneurysms • Iliac - 41% • Femoro-popliteal - 15% • Pts with unilateral popliteal aneurysms-->8% AAA • Pts with bilateral popliteal aneurysms--> 30%-50% AAA
Aortic AneurysmsAssociated Medical Conditions • Carotid Artery Stenosis - 10% have AAA • Smoker:Nonsmoker - 8:1 • Male:Female - 4:1 • HTN - 40% of pts with AAA have HTN
Aortic AneurysmsEtiology • Atherosclerosis • Cystic Medial Necrosis • Dissection • Ehlers-Danlos Syndrome • Syphilis • Familial Associated • Lysyl Oxidase deficiency
Aortic AneurysmsEtiology • Decrease in elastin and collagen in arterial wall • Elastin becomes fragmented-->arterial elongation and dilatation • Increase in the collagenase and elastase activity
Aortic AneurysmsEtiology Multifactorial
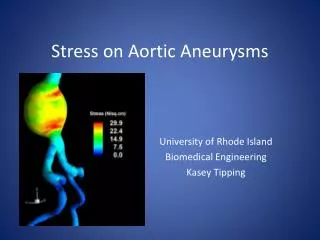
Aortic AneurysmsPhysics • Laplace’s Law T = P x R T - Tension P - Pressure R - Radius
Aortic AneurysmsClinical Presentation • Asymptomatic - 70-75% • Symptoms: • Early satiety, N,V • Abd., Flank, or Back pain • 1/3 of pts experience abd. And flank pain • Abrupt onset of pain -->Rupture or expansion of aneurysm
Aortic AneurysmsRuptured Aneurysms • Small tear-> pain, followed by frank rupture • Usually occurs postero-laterally • Can rupture in Vena Cava creating Aorto-Caval Fistula • Occasionally can rupture anterior - usually fatal
Ruptured AneurysmThumbnail Sketch • 60-70 y/o who presents with c/o abd pain, hypotension and a pulsatile abdominal mass
Aortic AneurysmsDiagnosis • Physical Exam: • If <5cm in diameter, then cannot be detected by routine physical exam • Radiographs: • Calcified wall. Can determine size in 2/3 • Cannot rule out and AAA
Aortic AneurysmsDiagnosis • Arteriography: • Cannot determine aneurysm size because of mural thrombus • Indications for obtaining arteriography • Suspicion of visceral ischemia • Occlusive disease of iliac and femoral arteries • Severe HTN, or impair renal function • ? Horseshoe Kidney • Suprarenal of TAAA component • Femoro-Popliteal Aneurysms
Aortic AneurysmsDiagnosis • Ultrasound • Establishes diagnosis easily • Accurately measures infrarenal diameter • Difficult to visualize thoracic or suprarenal aneurysms • Difficult to establish relationship to renal arteries • Technician dependent • Widely available, quick, no risk, cheap
Aortic AneurysmsCT Scan • Very reliable and reproducible • Can image entire aorta • Can visualize relation ship to visceral vessels • Longer to obtain and is more costly than U/S • Most useful • Requires contrast agent - renal toxicity
Aortic AneurysmsMRA • Now widely available • More expensive than CT • No contrast agent required • Spacial resolution less than CT
Aortic AneurysmsRisks • Complications of AAA • Thrombosis • Distal embolization • Rupture 23.4% of aneurysms 4-5 cm will rupture
Aortic AneurysmsRupture Risks • Patients with COPD and HTN have increased risk of rupture • Rate of enlargement: • 0.5 cm/ year • Survival • 50% die prior to reaching hospital, and an additional 24% prior to repair.
Aortic AneurysmsTreatment Risks • Mortality • 0.9 - 5% with current surgical techniques • Morbidity • 5-10% usually associated with cardiac events • Endovascular Techniques are significantly reducing morbidity and mortality associated with repair
Aortic AneurysmsIndications for Treatment • Presence of an infrarenal aneurysm > 5cm without associated co-morbid medical conditions • Repair smaller aneurysms if rate of enlargement is greater than expected • Repair all symptomatic aneurysms • If co-morbid conditions exist wait until risk of repair and rupture are equal (approx. 6 cm)
Aortic AneurysmsTreatment-Surgical • Standard Surgical Repair • Replace diseased aorta with artificial artery • Requires 7 day hospital stay • Recovery time 3-6 months • Proven method with good long term results
Aortic AneurysmsTreatment - Endovascular • Repair through an incision in the groin with expandable prosthesis under fluoroscopic guidance • Requires both surgical and radiological assistance • Significantly reduced m+m • Long tern result unknown • Hospital stay 2 days, Recovery time 1-2 weeks