Download
1 / 16
160 likes | 339 Views
Ontological analysis of SNOMED CT. Gergely H éja MSc. , Gy örgy Surjá n MD. , P éter Varga MSc. National Institute for Strategic Health Research , Budapest, Hungary. Aims. ESKI needs a reference terminology To represent of classification systems (ICD, ICPM) and public health indicators

E N D
Ontological analysis of SNOMED CT Gergely Héja MSc., György Surján MD., Péter Varga MSc. National Institute for Strategic Health Research, Budapest, Hungary Gergely Héja - SMCS2006
Aims • ESKI needs a reference terminology • To represent of classification systems (ICD, ICPM) and public health indicators • To provide pre co-ordinated code lists for enabling semantic interoperability in Hungary (and potentially in the EU) • SNOMED CT seems to be a first choice candidate Gergely Héja - SMCS2006
Needs for classification systems • Combinatory representation of categories based on a reference ontology to enable • supporting statistical analysis • formal consistency checking • (semi)automatic interconnection of different classification systems (e.g. ICD and ICPM) • A high-quality formal ontology is needed, but it needs not to be very detailed Gergely Héja - SMCS2006
Needs for interoperability • Detailed common terminology covering the whole domain of medicine • Mapping the concepts of the HIS to the concepts of the common terminology and vice versa • A common, consistent, comprehensive and decidable ontology is needed Gergely Héja - SMCS2006
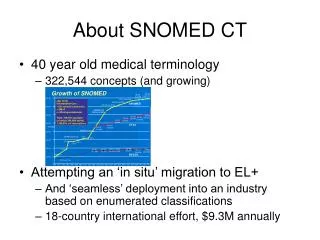
Computational issues • Computability vs. comprehensiveness • Clean hierarchies • Less emphasis on coverage (the multitude of non-defined leaf categories) and greater emphasis on rich and well-organized high-level categories is needed • SNOMED CT contains too much concepts Gergely Héja - SMCS2006
Methods • Based on DOLCE formal top-level ontology • Review of high and low-level concepts needed for the representation of classification systems and public health indicators • Is the subsumption relation valid? • Meaning derived from the FSN vs. meaning derived from synonyms vs.meaning derived from formal definition Gergely Héja - SMCS2006
Error types - 1 • Misplacing concepts in the hierarchy • smoker (an agent) is subsumed by tobacco smoking behaviour – finding (a role) • severe asthma is not a kind of asthma, but a kind of asthma finding. • Mixing the subsumption relation with other roles (typically part of) • haemoglobin subsumes haemin (instead of constitutional part) • exacerbation of asthma attack is subsumed by asthma (instead of temporal part) Gergely Héja - SMCS2006
Error types - 2 • Hierarchy violating medical thinking and biomedical knowledge • Disease, observation and finding are subsumed by clinical finding • acute on chronic, which is both subsumed by acute and chronic • polycarbonate is a polymer (instead of synthetic polymer) Gergely Héja - SMCS2006
Error types - 3 • Contracting disjoint entities into one concept • Smoker (an agent) and smoker (finding) (a description of a situation) • additional pathologic finding in tumor specimen (observable entity) and additional pathologic finding • Function is classified as an observable entity • Ontological definition: ability of an object to play a certain role in a certain kind of activity • functions (e.g. gene function,adaptation) • measures (quality) that evaluate the realisation of a function (e.g. respiratory rhythm, excretory rate) • Inflammation (morphological abnormality) (a physical object) and inflammatory reaction (perdurant) Gergely Héja - SMCS2006
Additional problems - 1 • Categories taken form classification systems • pneumonia in other diseases classified elsewhere (marked as “ConceptStatus Limited”) • The danger of taking over concepts from other conceptual systems: the context of the concept is lost. What is meant by “other diseases classified elsewhere”? • relations (such as part of) are represented also as concepts • It prohibits the direct conversion to any formalism based on first order logic, thus to any DL formalism Gergely Héja - SMCS2006
Additional problems - 2 • Underspecification: • roles are not quantified (existential / universal) • criteria are not specified (necessary / sufficient) • conversion to DL: do we have to decide in each particular case, or can it be done universally? • Multiple hierarchy • alcoholic beverage (through its parent ingestible alcohol) is subsumed by central depressant, ethyl alcohol and psychoactive substance of abuse – non-pharmaceutical. Alcoholic drinks contain ethyl alcohol, which plays a role of depressant and substance of abuse (with respect to human beings) • Is this a general phenomenon in SNOMED? • Which relations are asserted and which are inferred? Gergely Héja - SMCS2006
Discussion - 1 • The intended meaning of the categories is not always clear: possible translation errors • Is it reasonable to import categories from medical classifications? • Size • Artificial concepts • Consistency errors Gergely Héja - SMCS2006
Discussion - 2 • Real world entities listed heterogeneously • Mars bar and Kit Kat (chocolate candy would suffice) • UFO is subsumed by transport vehicle • tendon pulley reconstruction is represented, but tendon pulley not Gergely Héja - SMCS2006
Solutions • Use SNOMED as a plain or loosely structured list of terms (with extending the coverage). Not appropriate for intelligent services. • Restructure SNOMED into a high-quality ontology. • Build a new medical ontology from scratch (partial reuse of the existing ones), and to restrict the use of SNOMED for interoperability by mapping concepts to it. Gergely Héja - SMCS2006
Restructuring SNOMED • A formal top level ontology (e.g. DOLCE). • A high level core reference ontology of general medical knowledge (e.g. anatomy, physiology, pathology, medical procedures). • Logic-based formalism • Single hierarchies with formal definitions • (sub)domain ontologies of specialities • Compound entities (e.g. tonsillitis) • Manual assertion (e.g. autism) Gergely Héja - SMCS2006
Questions? Gergely Héja - SMCS2006