Download
1 / 118
1.18k likes | 1.2k Views
Learn the essential physiology of the central nervous system for anesthesia in neurosurgery. Explore neuroanatomy, neurophysiology, the blood-brain barrier, and autoregulation of cerebral blood flow.

E N D
CENTRAL NERVOUSSYSTEM DISEASE Dr Abdollahi
Anesthesia for neurosurgery requires an understanding of the physiology of the central nervous system (CNS). The anesthesia provider must control the physiologic and pharmacologic factors that influence cerebral blood flow (CBF), cerebral metabolic rate for oxygen consumption (CMR02), and intracranial pressure (ICP). The selection of drugs, ventilation techniques, and monitors have important implications in the care of patients with diseases of the CNS.
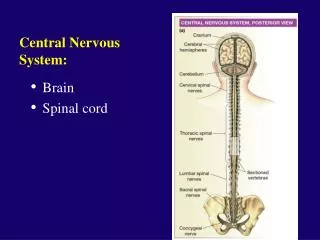
NEUROANATOMY • Conceptually, the cranium is divided into supratentorial and infratentorial compartments. The supratentorial compartment contains the cerebral hemispheres and diencephalon • (thalamus and hypothalamus); the brainstem and cerebellum make up the infratentorial compartment.
The location of intracranial pathology can have significant • implications, particularly if eloquent areas such as the language • centers and motor cortex of the brain are at risk.
Arterial blood supply • The arterial blood supply to the brain is through the left and right internal carotid arteries and the vertebrobasilar system. Anastomoses between these vessels form the circle • of Willi and create a collateral blood supply to protect against ischemia. The classic depiction of this ring is found in fewer than half of human brains and collateralization may not be complete in all individuals.
Blood-brain barrier (BBB) • Many of the physiologic properties of the central nervous system are dependent on an intact blood-brain barrier. The blood-brain barrier is composed of capillary endothelial cells with tight junctions that prevent extracellular passage of macromolecules, such as proteins.
In contrast, lipid-soluble substances (carbondioxide, oxygen, anesthetics) cross the blood-brain barrier easily. The blood-brain barrier may be disrupted in the event of acute systemic hypertension, trauma, infection, arterial hypoxemia, severe hypercapnia, tumors, and sustained seizure activity.
NEUROPHYSIOLOGY • Cerebral Blood Flow • Normal CBF is approximately 50 mL/100 g/min and represents 15% of cardiac output. The brain receives a disproportionately large share of cardiac output due to its high metabolic rate and inability to store energy.
Determinants of CBF include • (1) CMR02, • (2) cerebral perfusion pressure (CPP) and autoregulation, • (3) PaC02 • (4) Pa02 • (5) Anesthetic drugs • The impact of autonomic system innervation on CBF is small.
Cerebral Metabolic Rate • Cerebral blood flow in the brain is heterogeneous and directly influenced by CMR02 through cerebral flow metabolism • coupling. Increases or decreases in CMR02 result in a proportional increase or decrease in CBF.
CMR02 is reduced by hypothermia and most anesthetic drugs and produces a coupled reduction in CBF in healthy brains (CBF decreases 7% for every 1 o C decrease in body temperature below 37° C). In contrast, CMR02 and CBF may be dramatically increased by seizure activity.
Cerebral Perfusion Pressure andAutoregulation • CPP is the difference between mean arterial pressure (MAP) and ICP or central venous pressure (CVP), whichever is greater. Autoregulation is a protective mechanism that maintains a constant CBF in the presence of a changing CPP and reflects the ability of cerebral arterioles to constrict or relax in response to changes in perfusion pressure.
This response normally requires 1 to 3 minutes to develop, so a rapid increase or decrease in MAP causes a brief period of cerebral hyperperfusion or hypoperfusion, respectively
Autoregulation maintains CBF relatively constant between a CPP of 50 and 150 mm Hg in normotensive, healthy individuals. • Cerebral blood flow varies directly with cerebral perfusion pressures above or below this range. Chronic uncontrolled hypertension or sympathetic stimulation shifts the autoregulatory curve to the right, and these patients require a higher minimum CPP to maintain adequate CBF.
The anesthetic state shifts the autoregulatory response to the left, which may provide some safety from the decreases in MAP that can occur intraoperatively.
Autoregulation may be impaired in specific circumstances. • Autoregulation can be abolished following traumatic brain injury and intracranial surgery. As a result, CBF becomes directly proportional to MAP which has important clinical implications in the management of these patients.
Autoregulation may also be impaired in the proximity of intracranial tumors. Inhaled anesthetics are potent cerebral vasodilators and impair autoregulationto varying degrees at high doses.
Although autoregulation is maintained at anesthetic concentrations less than 1 minimum alveolar concentration (MAC) higher concentrations abolish autoregulation, and CBF becomes proportional to MAP. In contrast, intravenous anesthetics do not disrupt autoregulation.
Effects of PaC02 and Pa02 on CBF • Changes in PaC02 produce corresponding directional changes in CBF between a PaC02 of 20 to 80 mm Hg CBF increases or decreases 1 mL/100 g/min for every 1-mm Hg increase or decrease in PaC02 from 40 mm Hg.
Such changes in CBF reflect the effect of carbon dioxide-mediated alterations in perivascular pH and lead to dilation or constriction of cerebral arterioles.These changes in CBF are transient because of an increase in cerebrospinal fluid (CSF) HC03 concentrations.
CBF returns to normal in 6 to 8 hours, even if the altered PaC02 • levels are maintained.Aggressive or prolonged hyperventilation (PaC02 < 30 mm Hg) should be avoided because of the risk of cerebral ischemia. Prolonged aggressive hyperventilation following traumatic brain injury is probably associated with poorer neurologic outcome
Decreases in Pa02 (less than a threshold value of about • 50 mm Hg) result in an exponential increase in CBF.
Effect of Anesthetic on CBF • Intravenously administered anesthetics, such as thiopental, • propofol, and etomidate, are cerebral vasoconstrictors • and reduce CMR02 and CBF in parallel and are therefore • used frequently for anesthesia for neurosurgery. There is • controversy about the effects of ketamine, which probably • reflects differences in the conditions of the research study.
KETAMINE • When ketamine is given on its own without control of ventilation, PaC02, CBF, and ICP all increase, whereas when given in the presence of another sedative/ anesthetic drug in patients whose ventilation is controlled, these increases do not occur. Because of this controversy, however, ketamine is not usually selected for patients with known intracranial disease.
Benzodiazepines and opioids • Benzodiazepines and opioids decrease CMR02 and CBF, • analogous to thiopental and propofol, although to a lesser • extent. However, associated respiratory depression and elevation of PaC02 may produce the opposite effect.
Opioid • Opioids should be used with caution in patients with intracranial • disease because of their (1) depressant effects on consciousness, (2) production of miosis, and (3) depression of ventilation with associated increases in ICP from PaC02 increases.
a2-agonists • a2-agonists (clonidine and dexmedetomidine) are unique • sedatives in that they do not cause significant respiratory • depression. They reduce arterial blood pressure, CBF, • and CPP with minimal effects on ICP. a2-Agonists can be • used intraoperatively to reduce the dose of other anesthetics • and analgesics or postoperatively as sedatives and to attenuate • postoperative hypertension and tachycardia.
Volatile anesthetic • Volatile anesthetic drugs are potent cerebral vasodilators. • When administered during normocapnia at concentrations • higher than 0.5 MAC destlurane, sevoflurane, and isoflurane rapidly produce cerebral vasodilation and result in dose-dependent increases in CBF. CBF remains increased relative to CMR02 despite concomitant decreases in CMR02• • When used in isolation, nitrous oxide increases CBF and possibly CMR02, but these effects appear to be • attenuated by co-administration of other anesthetics.
INTRACRANIAL PRESSURE • Intracranial Pressure-Volume Relationship • The intracranial compartment is composed of three substances: • (1) brain matter, (2) cerebral spinal fluid, and (3) blood. Increases in any of the these substances can result in elevated intracranial pressure, defined as a sustained • increase above 15 mm Hg.
The pressure-volume compliance curve depicts the impact of increasing intracranial volume on intracranial pressure (ICP). As volume increases from point 1 to point 2 on the curve, ICP does not increase because cerebrospinal fluid is shifted from the cranium into the spinal subarachnoid space. Patients with intracranial tumors who are between point 1 and point 2 on the compliance curve are unlikely to manifest clinical symptoms of increased ICP. Patients who are on the rising portion of the pressure-volume curve (point 3) can no longer compensate for increases in intracranial volume, and ICP begins to increase. Clinical symptoms attributable to increased ICP are likely at this stage. Additional increases in volume at this point, as produced by increased CBF during anesthesia, can precipitate abrupt increases in ICP (point 4).
Effect of Anesthetic on ICP • Most intravenous anesthetic drugs reduce CMR02 and CBF, • and this decrease is associated with a reduction in ICP. The • effects of ketamine are controversial and were discussed • earlier. These drugs may be administered to patients with • intracranial hypertension to decrease ICP.
However, this must be done carefully as large doses of propofol or thiopental may decrease systemic blood pressure and CPP. An increased frequency of excitatory peaks on the electroencephalogram of patients receiving etomidate, as compared with thiopental, suggests caution in the administration of etomidate to patients with a history of epilepsy
Opioids and benzodiazepines reduce ICP through reductions in CBF and CMR02 although this benefit will be offset if respiratory depression and increases in PaC02 occur.
Cerebral vasodilators and produce dose-dependent increases • in ICP that parallel the increases in CBF and CBV. Hyperventilation to decrease PaC02 to less than 35 mm Hg attenuates the tendency for volatile anesthetics to increase ICP.
Neuromuscular blocking drugs do not usually affect ICP unless they induce release of histamine or hypotension. Histamine can cause cerebral vasodilation, leading to a small increase in ICP. Succinylcholine may increase ICP through stimulation of muscle spindles, which in tum either directly or indirectly results in increased CMR02.
NEUROPROTECTION • Many anesthetics may act as neuroprotectants given their potential to reduce cerebral metabolic rate and excitotoxicity during oxygen deprivation. In animal studies, many anesthetics, including barbiturates, volatile anesthetics, xenon, and propofol, provide neuroprotection although human outcome data are lacking. • Hypothermia has been described as a method for cerebral • protection during acute injury.
NEUROPHYSIOLOGIC MONITORING • Neurophysiologic monitoring is employed during neurosurgery with increasing frequency due to minimal risk to patients and the potential to reduce neurologic deficits. An understanding of the effects of anesthetic agents on somatosensory and motor evoked potentials is critical in neuroanesthesia. In general, nitrous oxide and volatile anesthetics have a greater effect on motor and sensory evoked potentials than intravenous anesthetics.
Electrocorticography • Electrocorticography (ECG) is another intraoperative mapping technique used to identify epileptic foci for resection and is • sensitive to anesthetic drugs that change the seizure threshold (e.g., benzodiazepines and volatile anesthetic agents).
Anesthesia For Neurosurgery • Preoperative Assessment • Patients presenting for neurosurgical procedures can have a • wide range of symptoms. Patients with intracranial mass lesions may present with seizures, altered level of consciousness, headaches, cranial nerve abnormalities, and motor or sensory deficits. Aneurysms and arteriovenous malformations (AVMs) can present with a severe ("thunderclap") headache if ruptured, and focal deficits or visual impairment from compression of the optic chiasm when unruptured.
Evidence of increased ICP should be elicited during the preoperative visit. Clinical signs may be consistent with • but do not reliably indicate, the level of ICP .
Imaging may reveal a midline shift of more than 0.5 cm, encroachment of expanding brain on cerebral ventricles, • cerebral edema, hydrocephalus, or any combination of these signs. In symptomatic patients, preoperative medications • that cause sedation or depression of ventilation are usually avoided.
Drug-induced depression of ventilation can lead to increased PaC02 and subsequent increases in ICP. In alert patients, small doses of benzodiazepines may provide useful relief of anxiety.
Monitoring • In addition to standard monitors, continuous monitoring of arterial blood pressure via a peripheral arterial catheter is recommended because of hemodynamic perturbations occurring during induction of anesthesia, tracheal intubation, • surgery, and emergence from anesthesia, all of which may compromise cerebral perfusion.
These catheters also allow for arterial blood gas sampling and accurate determination of PaC02.Central venous catheters are not routinely used and employed for patient indications, • such as anticipated need for vasoactive infusions. Measurement of the end-tidal carbon dioxide concentration • (capnography) is used to determine ventilation parameters.
The electrocardiogram (ECG) allows prompt detection of cardiac dysrhythmias caused by surgical manipulation of cardiovascular centers. Neuromuscular blockade is monitored with a peripheral nerve stimulator. • Because of the length of these surgical procedures and the use of diuretics, a bladder catheter is often necessary and helps in guiding intravenous fluid therapy. A continuous monitor of ICP is helpful but rarely used