Download
1 / 42
450 likes | 1.06k Views
I nterventions for Clients with Problems of the Thyroid and Parathyroid Glands. Hormones from the thyroid and parathyroid glands affect general metabolism, electrolyte balance, and excitable membrane activity.

E N D
Interventions for Clientswith Problems of the Thyroidand Parathyroid Glands
Hormones from the thyroid and parathyroid glands affect general metabolism, electrolyte balance, and excitable membrane activity. • Therefore a disturbance in either thyroid or parathyroid function usually has widespread clinical manifestations. • With mild disturbances, the problems are subtle. • With more severe disturbances, the problems may be life threatening
Hyperthyroidism • Excessive thyroid hormone secretion results in hyperthyroidism. • The clinical manifestations of hyperthyroidism are referred to as thyrotoxicosis. • Thyroid hormones affect all metabolic processes in all body organs and therefore produce numerous and varied clinical manifestations. • Hyperthyroidism can be temporary or permanent depending on the cause
Hyperthyroidism • Because thyroid hormones stimulate most body systems, excessive thyroid hormones produce a state of hypermetabolism with increased sympathetic nervous system activity • Thyroid hormones directly stimulate the heart. The increased heart rate and stroke volume in hyperthyroidism cause an increase in cardiac output and peripheral blood flow. • This excessive or hyperdynamic circulatory state results from an increase in the number of adrenergic receptors on the heart muscle
Hyperthyroidism • Elevated levels of thyroid hormones affect protein, carbohydrate, and lipid metabolism. • Protein synthesis (buildup) and degradation (breakdown) are increased. Breakdown exceeds buildup, causing a net loss of protein known as a negative nitrogen balance. Glucose tolerance is decreased, and the client has hyperglycemia (elevated blood glucose levels). • Fat metabolism is increased, which results in decreased body fat stores. Although the client has an increased appetite, food intake does not meet energy demands, and the client loses weight. With prolonged hyperthyroidism, the client is in a state of chronic nutritional deficiency
Hyperthyroidism • If hyperthyroidism is present before puberty, sexual development is delayed. • If hyperthyroidism develops after puberty, women experience menstrual irregularities and decreased fertility. • Both men and women with hyperthyroidism experience an increased libido (sexual urge or interest)
Hyperthyroidism • Age, gender, and usual weight are recorded. • The client may report a recent weight loss and an increased appetite. • Diarrhea is common. • A hallmark of hyperthyroidism is heat intolerance. The client may have diaphoresis (increased sweating) even when environmental temperatures are comfortable for others. The client often wears lighter clothing in cold weather. • The client may also report palpitations or chest pain as a result of the cardiovascular effects. • The nurse asks about changes in breathing patterns, because dyspnea (with or without exertion) is common
Hyperthyroidism • Visual changes may be the earliest problem noted in the client with hyperthyroidism, especially ophthalmopathy with Graves' disease. • The client is asked about changes in vision, such as blurring or double vision and tiring of the eyes • Fatigue, weakness, and insomnia are common. • Family and friends may report that the client has become more irritable or depressed • Women are asked about changes in menses, because amenorrhea or a decreased menstrual flow is common
Hyperthyroidism. Assessment • Two types of ophthalmopathy (abnormal eye appearance or function) are common with hyperthyroidism: eyelid retraction (eyelid lag) and globe (eyeball) lag. • In eyelid lag, which occurs in all forms of thyrotoxicosis, the upper eyelid fails to descend when the client gazes slowly downward. • In globe lag, the upper eyelid pulls back faster than the eyeball when the client gazes upward • Infiltrative ophthalmopathy, which leads to exophthalmos, is common in clients with Graves' disease. • The wide-eyed or "startled" look is due to edema in the extraocular muscles and increased fatty tissue behind the eye, which pushes the globe forward. Pressure on the optic nerve may impair vision. Swelling and shortening of the muscles may cause problems with focusing. If the eyelid fails to close completely and the eye is unprotected, the eye may become overdry and prone to corneal ulceration or infection. • The nurse observes the client's eyes for excessive tearing and a bloodshot appearance and asks about sensitivity to light (photophobia)
Hyperthyroidism. Assessment • The nurse palpates the thyroid gland to determine the presence of a mass or general enlargement, observing the size and symmetry of the gland. In goiter, a generalized thyroid enlargement in people with Graves' disease, the thyroid gland may increase to four times its normal size. • Bruits (turbulence from increased blood flow) may be heard with a stethoscope. • The nurse inspects the client's hair and skin. Fine, soft, silky hair and smooth, moist skin are common with hyperthyroidism. • The client may have extremity muscle weakness, hyperactive deep tendon reflexes, or tremors. • Gross motor movements are observed for tremors, especially of the hands. • Reflexes may be hyperactive. The client may appear extremely restless, irritable, and fatigued
Hyperthyroidism. Assessment • The client with hyperthyroidism often experiences emotional lability (mood instability), irritability, decreased attention span, and manic behavior. • Mild to severe hyperactivity often leads to a state of fatigue because of the inability to sleep well. • The nurse asks the client whether he or she has been crying or laughing inappropriately or has had difficulty concentrating. • The client's family members or significant other often report these changes in mental or emotional status
Hyperthyroidism. Assessment • Thyroid scan • Ultrasonography • Electrocardiography
Hyperthyroidism. Interventions • The cardiac problems of hyperthyroidism include increased systolic blood pressure, a widened pulse pressure, tachycardia, and other dysrhythmias. • The goals of nonsurgical management are to decrease the effect of thyroid hormone on cardiac function and to reduce thyroid hormone secretion. • Surgery may be necessary when nonsurgical interventions are unsuccessful
Hyperthyroidism. Interventions Nonsurgical management • The nurse monitors the client's apical pulse, blood pressure, and temperature at least every 4 hours. The client is instructed to report any palpitations, dyspnea, vertigo, or chest pain immediately. • Fatigue is common, and the client is encouraged to rest. The environment is kept as quiet as possible. • Frequent bed linen changes, sponge baths, and a cool environment decrease discomfort caused by diaphoresis and heat intolerance
Hyperthyroidism. Interventions • Radioactive iodine (RAI) therapyis contraindicated in pregnant women because131I crosses the placenta and can adversely affect the fetal thyroidgland
Hyperthyroidism. Interventions Surgical management • Antithyroid drugs and RAI therapy are now the most common treatments for clients with hyperthyroidism. • Surgery to remove all or part of the thyroid gland may be necessary for clients who have a large goiter causing tracheal or esophageal compression or who are unresponsive to antithyroid drugs. • Removal of all (total thyroidectomy) or part (subtotal thyroidectomy) of the thyroid tissue decreases the production of thyroid hormones. • Clients undergoing a total thyroidectomy must take lifelong thyroid hormone replacement. • This surgery is also indicated in certain types of thyroid cancer
Hypothyroidism • Cellular energy production is decreased, and many metabolites build up. • The metabolites are compounds of proteins and sugars called glycosaminoglycans. • These compounds build up inside cells, which increases the mucous and water, forms cellular edema, and changes organ texture. The cellular edema is mucinous edema (called myxedema) rather than edema caused by water alone. • This edema changes the appearance of the client with full-blown hypothyroidism. Nonpitting edema forms everywhere and is especially evident around the eyes, in the hands and feet, and between the shoulder blades. • These same compounds cause the tongue to thicken and edema to form in the larynx, making the voice more husky. It is likely that these metabolites build up in other tissues and organs, decreasing general physiologic function
Hypothyroidism • Myxedema coma is a rare but serious complication of untreated or inadequately treated hypothyroidism. The decrease in metabolism in cardiac tissue causes the heart muscle to become flabby and the chamber size to increase. • The result is decreased cardiac output and decreased perfusion to the brain and other vital organs. • The decreased perfusion makes the already slowed cellular metabolism worse, resulting in tissue and organ failure. • The mortality rate for myxedema coma is extremely high, and this condition is considered a life-threatening emergency
Hypothyroidism Causes of mixedema coma
Hypothyroidism • HISTORY • A decrease in thyroid hormone produces a variety of signs and symptoms related to decreased metabolic activity. • The client often reports an increase in time spent sleeping, sometimes up to 14 to 16 hr/day. The client may also have generalized weakness, anorexia, muscle aches, and paresthesias. • Constipation is common. • The client often has cold intolerance, and the nurse asks if more blankets at night or sweaters and extra clothing in warm weather have been needed. • Both male and female clients may identify a decrease in libido. In addition, women with hypothyroidism may have had difficulty becoming pregnant or experienced changes in menses (heavy, prolonged bleeding or amenorrhea). • Men can have problems with impotence and fertility
Hypothyroidism • The client is asked about his or her current or previous use of medications, such as lithium, aminoglutethimide, sodium or potassium perchlorate, thiocyanates, or cobalt. All of these drugs can impair the production of thyroid hormone. • The client is asked whether he or she is taking any tranquilizers or opioids (hypothyroidism increases the sensitivity to these drugs as a result of decreased metabolism)
Hypothyroidism • MYXEDEMA COMA • The following problems are associated with this condition: • Coma • Respiratory failure • Hypotension • Hyponatremia • Hypothermia • Hypoglycemia • Untreated myxedema coma leads to shock, organ damage, and death. • The nurse assesses the client with hypothyroidism every shift for changes that indicate increasing severity of hypothyroid symptoms, especially changes in mental status.
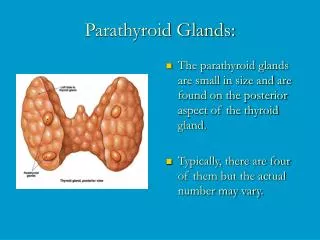
Hyperparathyroidism • The parathyroid glands maintain calcium and phosphate balance. • Increased levels of parathyroid hormone (PTH) act directly on the kidney, causing increased kidney reabsorption of calcium and increased phosphate excretion. • These processes cause hypercalcemia (excessive calcium) and hypophosphatemia (inadequate phosphate) in the client with hyperparathyroidism. • In the bone, excessive PTH levels increase bone resorption (bone loss of calcium) by decreasing osteoblastic (bone production) activity and increasing osteoclastic (bone destruction) activity. This process releases calcium and phosphate into the circulation and demineralizes bone. When the normal solubility of calcium in the serum is exceeded, as in long-standing hypercalcemia, calcium is deposited in soft tissues
Hyperparathyroidism Assessment • The nurse asks about the client's symptoms and any bone fractures, recent weight loss, arthritis, or psychologic distress. • Any history of radiation treatment to the head or neck is also obtained. The client with long-standing disease may have a waxy pallor of the skin and bone deformities in the extremities and back. • The clinical features of hyperparathyroidism may be related either to the effects of excessive PTH or to the effects of the accompanying hypercalcemia. • High levels of PTH cause renal calculi (kidney stones) and nephrocalcinosis (deposits of calcium in the soft tissue of the kidney). • Bone lesions are due to an increased rate of bone destruction and result in pathologic fractures, bone cysts, and osteoporosis in advanced cases. • Gastrointestinal manifestations (e.g., anorexia, nausea, vomiting, epigastric pain, constipation, and weight loss) are common, particularly when serum calcium levels are high. Hypergastrinemia (elevated serum gastrin levels) is caused by hypercalcemia and leads to peptic ulcer disease. • Fatigue and lethargy may be present and become more severe as the serum calcium levels increase. When serum calcium levels are greater than 12 mg/dL, the client may have psychosis with mental confusion, which leads to coma and death if left untreated
Hyperparathyroidism • Serum PTH, calcium, and phosphate levels and urine cyclic adenosine monophosphate (cAMP) are the most commonly used laboratory tests to detect hyperparathyroidism • X-rays may show kidney stones, calcium deposits, and bone lesions, such as cysts or fractures. Generalized bone demineralization and resorption in the long bones occur in the client with chronic hyperparathyroidism. • Other diagnostic tests include arteriography, computed tomography (CT), venous catheterization of the thyroid veins with sampling of the blood for PTH levels, and ultrasonography. • The nurse explains the procedures and cares for the client undergoing diagnostic tests
Hyperparathyroidism Interventions • Nonsurgical management • Diuretic and fluid therapy. • The most common therapy for reducing serum calcium levels in clients who are not candidates for surgery is hydration and furosemide, a diuretic that increases kidney excretion of calcium. • IV saline in large volumes also promotes renal calcium excretion. • The nurse monitors cardiac function and intake and output every 2 to 4 hours during hydration therapy. Continuous cardiac monitoring may be required. • The nurse closely monitors serum calcium levels and immediately reports any precipitous drop to the physician. Sudden drops in calcium levels may cause tingling and numbness in the muscle
Hyperparathyroidism • Drug therapy. • When hydration and furosemide cannot reduce hypercalcemia, or if it becomes necessary to discontinue IV fluids, additional medications can help to reduce the clinical manifestations of hyperparathyroidism, especially those related to hypercalcemia. • Phosphates. Oral phosphates inhibit bone resorption and interfere with calcium absorption. IV phosphates are used only when serum calcium levels must be lowered rapidly. • Calcitonin. Calcitonin decreases skeletal calcium release and increases the kidney excretion of calcium. Calcitonin is not effective when used alone because of its short duration of action. Its therapeutic effects are greatly enhanced if given in conjunction with glucocorticoids
Hyperparathyroidism • Calcium Chelators. Some drugs lower calcium levels by binding (chelating) calcium, which reduces the levels of free calcium. Mithramycin, a cytotoxic agent, is the most effective and potent calcium chelator used to lower serum calcium levels. • In most clients a single IV dose of 10 to 15 mg/kg of body weight by slow infusion can lower serum calcium levels within 48 hours. However, the toxic effects limit its use to two or three doses. Thrombocytopenia (decreased circulating platelets and an increased tendency to bleed) and kidney and liver toxicity can result after only one dose. Liver function studies, blood urea nitrogen and creatinine, complete blood count (CBC), and serum calcium levels are closely monitored in the client receiving mithramycin. Another calcium chelator is penicillamine (Cuprimine, Pendramine) • Surgical management. Surgical management of hyperparathyroidism involves a parathyroidectomy
Hypoparathyroidism • Hypoparathyroidism is an uncommon endocrine disorder in which parathyroid function is decreased. Problems are directly related to a lack of parathyroid hormone (PTH) secretion or to decreased effectiveness of PTH on target tissue. • Whether the problem is a lack of PTH secretion or an ineffectiveness of PTH on tissues, the result is the same — hypocalcemia. • Iatrogenic hypoparathyroidism, the most common form, is caused by the removal of all parathyroid tissue during total thyroidectomy or by deliberate surgical removal of the parathyroid glands.
Hypoparathyroidism • Idiopathic hypoparathyroidism is a rare condition that can occur spontaneously. The exact cause is unknown, but an autoimmune basis is suspected because antiparathyroid antibodies are present in many affected clients. In addition, hypoparathyroidism is often associated with the following autoimmune disorders: adrenal insufficiency, hypothyroidism, diabetes mellitus, pernicious anemia, gonadal failure, and vitiligo. • Hypomagnesemia (decreased serum magnesium levels) may also cause hypoparathyroidism. Hypomagnesemia is seen in alcoholics and in clients with malabsorption syndromes, chronic renal disease, and malnutrition. It causes impairment of PTH secretion and may interfere with PTH effects on the bones and kidneys
Hypoparathyroidism Assessment • The nurse begins assessment of the client with suspected hypoparathyroidism by asking about any head or neck surgery or radiation therapy, because these treatments may cause hypoparathyroidism. • The client is asked about the signs and symptoms of hypoparathyroidism, which may range from mild tingling and numbness to tetany. Tingling and numbness around the mouth or in the hands and feet reflect mild to moderate hypocalcemia. Severe muscle cramps, carpopedal spasms, and seizures (with no loss of consciousness or incontinence) reflect a more severe hypocalcemia. The client or caregiver may notice mental changes ranging from irritability to psychosis
Hypoparathyroidism • The physical assessment may show excessive or inappropriate muscle contractions that cause finger, hand, and elbow flexion; this can signal an impending attack of tetany. • The nurse checks for Chvostek's sign and Trousseau's sign; positive responses indicate potential tetany. • A parkinsonian-like syndrome may be evident. • The presence of cataracts denotes chronic hypocalcemia. • Bands or pits may encircle the crowns of the teeth, which indicates a loss of calcium from the teeth and causes enamel loss. The roots of the client's teeth may be defective
Hypoparathyroidism • Diagnostic tests for hypoparathyroidism include electroencephalography (EEG), blood tests, and computed tomography (CT). • EEG changes are nonspecific and revert to normal with correction of hypocalcemia. Serum calcium, phosphate, magnesium, vitamin D, and urine cyclic adenosine monophosphate (cAMP) levels may be used in the diagnostic workup for hypoparathyroidism. • The CT scan can show brain calcifications, which indicate chronic hypocalcemia
Hypoparathyroidism Interventions • Management of hypoparathyroidism focuses on correcting hypocalcemia, vitamin D deficiency, and hypomagnesemia. • For clients with acute and severe hypocalcemia, IV calcium is administered as a 10% solution of calcium chloride or calcium gluconate over 10 to 15 minutes. • Acute vitamin D deficiency is treated with calcitriol (Rocaltrol), 0.5 to 2.0 mg/day. • Acute hypomagnesemia is corrected with 50% magnesium sulfate in 2-mL doses (up to 4 g/day) either intramuscularly or intravenously. • Long-term oral therapy for hypocalcemia involves the administration of calcium, 0.5 to 2.0 g/day in divided doses. • Long-term therapy for vitamin D deficiency is 50,000 to 400,000 units of ergocalciferol daily. The dosage is adjusted to keep the client's calcium level in the low-normal range (slightly hypocalcemic), enough to prevent symptoms of hypocalcemia. It must also be low enough to prevent increased urine calcium concentrations, which can lead to stone formation
Hypoparathyroidism • Nursing management includes teaching about the medication regimen and interventions to reduce anxiety. • The client is instructed to eat foods high in calcium but low in phosphorus. • Milk, yogurt, and processed cheeses are avoided because of their high phosphorus content. • The nurse stresses that therapy for hypocalcemia is lifelong. The client is advised to use some form of identification, such as a Medic Alert bracelet or a wallet card. • With adherence to the prescribed drug and diet regimen, the calcium level usually remains high enough to prevent a hypocalcemic crisis