Download
1 / 59
590 likes | 771 Views
Vaccination of Adolescents. Andrew Kroger National Center for Immunization and Respiratory Diseases. National Assembly on School-based Health Care (NASBHC). Disclosure. The speaker is a U.S. government employee and has no conflict or interest with any manufacturer of products

E N D
Vaccination of Adolescents • Andrew Kroger • National Center for Immunization and Respiratory Diseases • National Assembly on School-based Health Care (NASBHC)
Disclosure • The speaker is a U.S. government employee and has no conflict or interest with any manufacturer of products • The speaker will discuss the use of Tdap in a manner that varies from the package insert
The 11-12 Year Old Visit • The recommended age for certain vaccines • An opportunity to catch-up on lapsed vaccinations
Adolescent Vaccines • Recommended • Tdap or Td • Meningococcal Conjugate • Human Papillomavirus • Catch-up • Hepatitis B • MMR • Varicella • Polio • Risk Groups • Pneumococcal Polysaccharide • Influenza • Hepatitis A • Meningococcal Polysaccharide
Pertussis Clinical Features • Stages • Incubation period – 5-10 days (21 days rare) • Catarrhal Stage – 1-2 weeks • Paroxysmal Stage – 1-6 weeks (10 days rare) • Convalescent stage – 2-3 weeks
Pertussis Clinical Features • Complications • Secondary bacterial infection pneumonia • More often in infants < 6 months • Seizures, otitis media, anorexia, dehydration • Complications from actual coughing: choking, epistaxis, subdural hematoma, hernia, rib fractures, rectal prolapse
Adolescent Pertussis Vaccination Objectives • Primary • Protect vaccinated adolescents • Secondary • Reduce B. pertussis reservoir • Potentially reduce incidence of pertussis in other age groups
Tdap Vaccines • AdacelTM (sanofi pasteur) • Licensed June, 2005 • Approved for persons 11-64 years of age • Boostrix® (GlaxoSmithKline) • Licensed May, 2005 • Approved for persons 10-18 years of age
General Principles for Use ofTdap and Td Among Adolescents • Tdap products are interchangeable • Tdap preferred to Td to provide protection against pertussis • Licensed only for a single dose at this time • Tdap not approved or recommended for children 7-9 years of age
ACIP Recommendations for Tdap Vaccines • Adolescents 11-12 years of age should receive a single dose of Tdap instead of Td* • Adolescents 13-18 years who have not received Tdap should receive a single dose of Tdap as their catch-up booster instead of Td* *if the person has completed the recommended childhood DTaP vaccination series, and has not yet received a Td booster
ACIP Recommendations for Tdap Vaccines • ACIP encourages adolescents who received a Td booster to receive a single dose of Tdap to provide protection against pertussis* • A 5-year interval between the Td and Tdap is encouraged to reduce the chance of a local reaction *if the person has completed the recommended childhood DTaP vaccination series
Minimum Interval Between Td and Tdap • ACIP did not define an absolute minimum interval between Td and Tdap • Provider will need to decide based on whether the benefit of pertussis immunity outweighs the risk of a local adverse reaction
Tdap For Persons Without AHistory of DTaP • All adolescents should have documentation of having received a series of DTAP, DTP, DT, or Td • Persons without documentation should receive a series of 3 vaccinations • Preferred schedule: • Single dose of Tdap* • Td at least 4 weeks after the Tdap dose • Second dose of Td at least 6 months after the Td dose *off-label recommendation
Tdap Contraindications • Severe allergic reaction to a vaccine component or following a prior dose • Encephalopathy within 7 days of administration of a pertussis vaccine that is not attributable to another identifiable cause
Tdap Precautions • History of an Arthus-type reaction following a previous dose of tetanus- or diphtheria-containing vaccine • Progressive neurological disorder, uncontrolled epilepsy, or progressive encephalopathy • History of Guillain-Barré syndrome (GBS) within 6 weeks after a previous dose of tetanus toxoid-containing vaccine • Moderate or severe acute illness
Conditions NOT Precautionsfor Tdap • Following a dose of DTaP/DTP: • Temperature 105o F (40.5o C) or higher • Collapse or shock-like state • Persistent crying lasting 3 hours or longer • Convulsions with or without fever • History of an extensive limb swelling reaction
DTaP and Tdap Administration Errors Error DTaP given to person >7 years Tdap given to child <7 years as DTaP #1, 2, or 3 Tdap given to child <7 years as DTaP #4 or 5 Action Count dose as valid Do not count dose; give DTaP now Count dose as valid
Meningococcal Vaccine • Recommended for: • all persons at the preadolescent visit (ages 11-12 years) • persons about to enter high school (age 15 years) • college freshmen living in a dormitory • other adolescents who wish to reduce their risk for meningococcal disease MMWR 2005;54(RR-7)
Meningococcal Disease Among Young Adults, United States, 1998-1999 • 18-23 years old 1.4 / 100,000 • 18-23 years old not college student 1.4 / 100,000 • Freshmen 1.9 / 100,000 • Freshmen in dorm 5.1 / 100,000 Bruce et al, JAMA 2001;286;688-93
Meningococcal Vaccine • Recommended for certain high-risk persons: • military recruits • certain research and laboratory personnel • travelers to and U.S. citizens residing in countries in which N. meningitidis is hyperendemic or epidemic
Meningococcal Vaccine • Recommended for certain high-risk persons: • complement component deficiency • functional or anatomic asplenia • HIV infection (“should be considered”)
Menomune – ‘old’ 4 types – A,C,Y,W-135 Approved for >2 yrs of age 1 dose, selective revaccination Subcutaneousinjection Menactra – new 4 types– A,C,Y,W-135 Approved for 11-55 years of age 1 dose, (currently) no revaccination Intramuscular injection Meningococcal Vaccines
Meningococcal Conjugate VaccineContraindications and Precautions • Contraindications • Severe allergic reaction to vaccine component or following prior dose • Precautions • Moderate or severe acute illness • Menactra: prior history of Guillain-Barré if not extremely high risk for meningococcal disease
MCV: Extremely High Risk • Microbiologists routinely exposed to isolates of Neisseria meningitidis
Human Papillomavirus (HPV) Vaccine • A vaccine to prevent cervical cancer • Licensed for 9-26 year olds as: • Gardasil™– Merck- Quadrivalent HPV (Types 6, 11, 16, 18) L1 VLP Vaccine • Cervarix™- GlaxoSmithKline (GSK) pending licensure (Types 16 and 18)
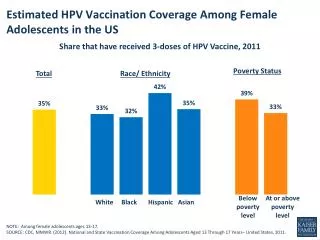
HPV Prevalence: Population Estimates, U.S. • 20 million people are infected • 6.2 million new infections each year • > 50% of sexually active men & women acquire genital HPV infection • 74% of new infections occur in persons 15 – 24 years of age W. Cates, STD April 1999, Weinstock, Perspectives on Sexual and Reproductive Health 2004, Koutsky Am J Med 1997
Human Papillomavirus >100 types Mucosal Cutaneous (~40types) (~60 types) “Common” “high-risk” “low-risk” warts types (16,18) types (6,11) (hands/feet) • low grade cervical abnormalities • high grade abnormalities/ • cancer precursors • anogenital cancers • low grade cervical abnormalities • genital warts • respiratory papillomas
Background: HPV-associated Conditions HPV types 16, 18, 6, 11 • Clifford GM, BJ Ca 2003, Munoz Int J Cancer 2004; Brown J Clin Micro 1993; Carter Cancer Res 2001; • Clifford Cancer Epi Biomarkers Prev 2005; Gissman Proc Natl Acad Science 1983; • Kreimer Cancer Epidemiol Biomarkers Prev. 2005 • * All oncogenic types
Cervical Cancer Mortality Rates U.S., 1946-1984 Source: Program for Improving Clinical Pap Smear Programs and Management, Office of Population Affairs, DHHS, 1987.
Efficacy for Prevention of Clinical HPV Disease Due to HPV 6/11/16/18* *Integrated dataset; results in the Per-Protocol Populations
Antibody Titers by Age at Enrollment Anti-HPV 6 GMTs (Quadrivalent HPV vaccine) Efficacy Program Immunogenicity Bridge 1600 1500 1300 1100 900 Serum GMT with 95% CI, mMU/mL 700 500 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 Age at Enrollment (Years) Merck, unpublished data, ACIP presentation by Eliav Barr, February 2006
Potential Unintended Consequences of HPV Vaccine • Research shows generally low levels of HPV knowledge • Multiple influences on adolescent sexual behavior • Fear of STD not apparent major motivation for abstinence • Increase in sexual risk unlikely
Pediatricians’ Intention to Recommend HPV Vaccine for Female and Male Patients, by Age Kahn J et al. Journal of Adolescent Health 2005
Quadrivalent HPV VaccineSummary • High efficacy in 16 to 26 year-old females who are naïve to the HPV vaccine type • HPV 16,18 related CIN 2/3 • HPV 6,11,16,18 related CIN • HPV 6,11,16,18 related external genital lesions • No evidence of efficacy against disease in persons already infected with relevant type • Efficacy data available through 5; duration of protection and need for booster unknown • Safe; side effects mainly local reactions
Recommendations • Routine vaccination • Catch-up vaccination • Special situations • Precautions and contraindications
Routine VaccinationRecommendation • ACIP recommends routine vaccination of females 11-12 years of age with three doses of quadrivalent HPV vaccine • The vaccination series can be started as young as 9 years of age
Rationale: Routine Vaccination Females at 11-12 Years • Routine • Prevalent infection, targeting ‘high risk’ groups not possible • Modeling shows greater impact • 11-12 years • Vaccination prior to sexual debut • Implementation advantages; consistent with young adolescent health care visit • High antibody titers after vaccination at this age • Data through 5 years show no evidence of waning immunity; ongoing studies will monitor duration of protection