1 / 4
40 likes | 83 Views
Get this template plus 350 other premium business tools & templates at www.demandmetric.com

E N D
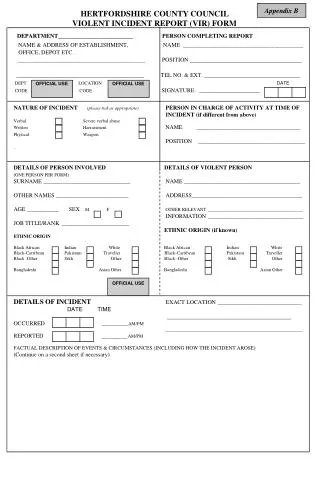
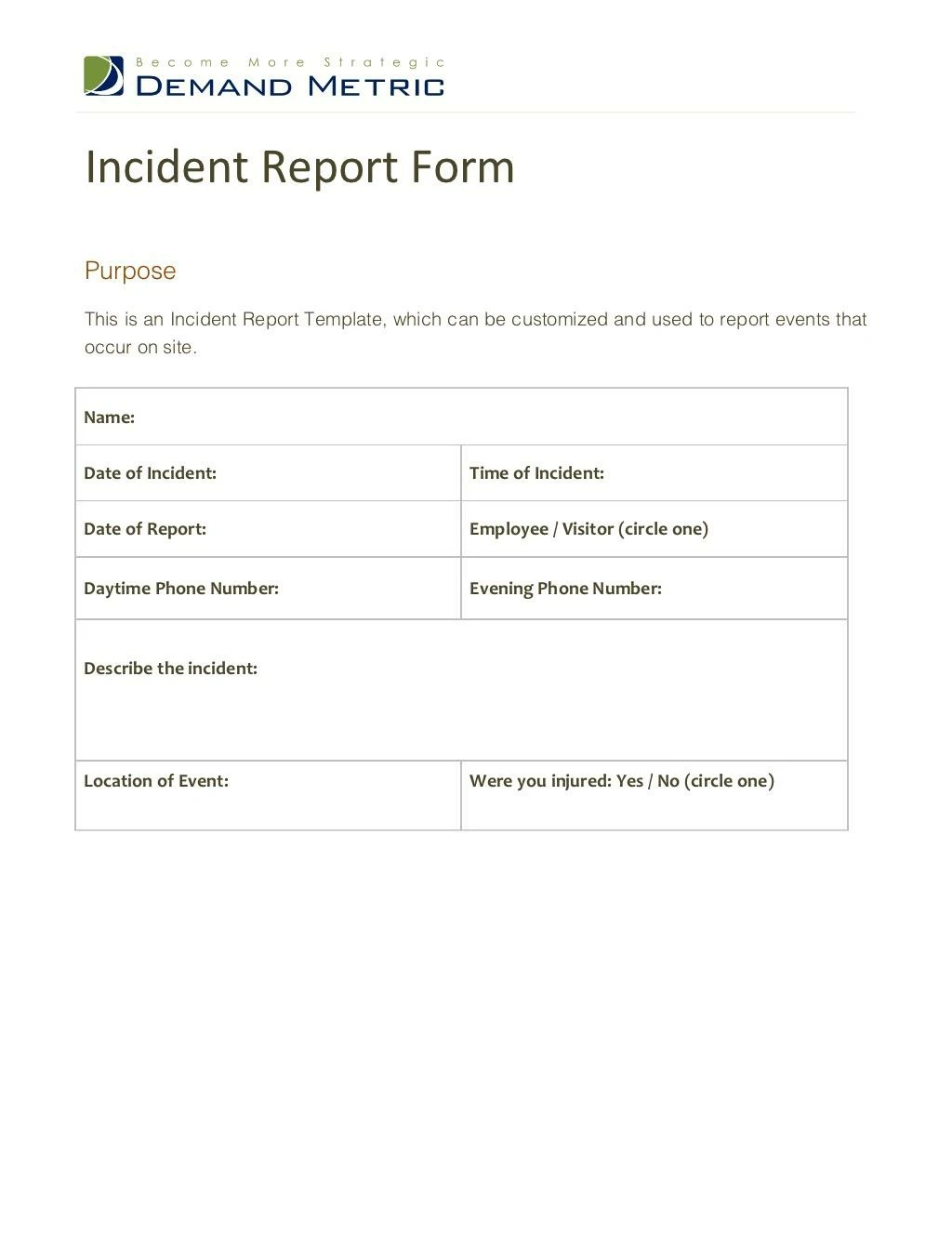
Incident Report Form Incident Report FormPurposeThis is an Incident Report Template, which can be customized and used to report events thatoccur on site.Name:Date of Incident: Time of Incident:Date of Report: Employee / Visitor (circle one)Daytime Phone Number: Evening Phone Number:Describe the incident:Location of Event: Were you injured: Yes / No (circle one)
(Please circle the areas of the body involved in theincident):Write a Description of the Injury:What factors contributed to the event?How could the event have been avoided?Was First aid administered? YES / NO If yes, by whom?Signature of Injured Party:Complainant Date:INJURED PARTY/COMPLAINANT TO COMPLETE, SIGN, DATE & SUBMIT toyour immediate supervisor/department within 24 HOURS of the event.If form completed by someone other than the injured party, please fill out the following lines:Form Completed by:Telephone Number: (Please circle the areas of the body involved in theincident):Write a Description of the Injury:What factors contributed to the event?How could the event have been avoided?Was First aid administered? YES / NO If yes, by whom?Signature of Injured Party:Complainant Date:INJURED PARTY/COMPLAINANT TO COMPLETE, SIGN, DATE & SUBMIT toyour immediate supervisor/department within 24 HOURS of the event.If form completed by someone other than the injured party, please fill out the following lines:Form Completed by:Telephone Number:
Signature Date:The IMMEDIATE SUPERVISOR IS TO COMPLETE, SIGN, DATE & SEND hardcopy to the Corporate Office. IF an injury occurred, SEND a copy to Benefits Office.Supervisor’s Name:Date of Incident: Time of Incident:Date of Report: Supervisor’s Position:Daytime Phone Number: Evening Phone Number:If there was a delay in reporting this event, list reason(s):Material Damage: YES / NO Approximate Value:Cause of event – List Root Causes:What corrective actions are being taken to prevent recurrence?Has a risk assessment been carried out for the process/activity? YES NOHave person(s) involved received training or instruction in the work or activity being carried out?YES / NO Signature Date:The IMMEDIATE SUPERVISOR IS TO COMPLETE, SIGN, DATE & SEND hardcopy to the Corporate Office. IF an injury occurred, SEND a copy to Benefits Office.Supervisor’s Name:Date of Incident: Time of Incident:Date of Report: Supervisor’s Position:Daytime Phone Number: Evening Phone Number:If there was a delay in reporting this event, list reason(s):Material Damage: YES / NO Approximate Value:Cause of event – List Root Causes:What corrective actions are being taken to prevent recurrence?Has a risk assessment been carried out for the process/activity? YES NOHave person(s) involved received training or instruction in the work or activity being carried out?YES / NO
Was there any supervision of the work or activity being carried out? YES / NOSupervisor’s Comments (Additional information on event):If injury occurred, please check one:o No First-Aid administered, returned to worko First-Aid administered, returned to worko Saw a physician, returned to worko Saw a physician, returned to light dutyo Saw a physician, time losso Refused medical treatmentSupervisor’s Signature:Date:Section C: General InformationDistribution: Risk Management Benefits Office, HR Department, Department Head, SeniorManagement.Follow-Up: Injured Party, Supervisor and Department HeadOther ____________ Other ____________ Was there any supervision of the work or activity being carried out? YES / NOSupervisor’s Comments (Additional information on event):If injury occurred, please check one:o No First-Aid administered, returned to worko First-Aid administered, returned to worko Saw a physician, returned to worko Saw a physician, returned to light dutyo Saw a physician, time losso Refused medical treatmentSupervisor’s Signature:Date:Section C: General InformationDistribution: Risk Management Benefits Office, HR Department, Department Head, SeniorManagement.Follow-Up: Injured Party, Supervisor and Department HeadOther ____________ Other ____________