Download
1 / 35
350 likes | 369 Views
Learn about the American Fitness Index program by ACSM, aiming to improve community health by promoting physical activity, preventive behaviors, and community support. The program collects, aggregates, and reports data to assess the health status of major metro areas, promoting a healthier lifestyle. Advisory board of experts guides the program components and implementation. Explore the methodology and indicators selected to assess health status and physical activity levels. Download data reports for pilot and expansion phases from the official website.

E N D
ACSM American Fitness Index™Actively Moving America to Better Health A program of the American College of Sports Medicine (ASCM)Presentation by First Last, Ph.D, FACSM Mo/Da/2009
ACSM American Fitness Index™ • Funded by the WellPoint Foundation • Looks at health status of population • Preventive health behaviors • Levels of chronic disease conditions • Access to health care • Looks at community assets that support healthy lifestyles • Community supports • Policies for physical activity
Need for Action • Physical activity and obesity are at epidemic proportions • Increased prevalence of chronic diseases • Increasing health expenditures • Regular physical activity • Therapeutic physical benefits • Fewer health care needs • Combats rising health care expenditures
Need for Action • ACSM-commissioned 2007 Omnibus survey • Solution to decreasing physical activity and obesity lies at the local level • Highlights: • 72% rated community’s efforts to encourage physical activity as average or worse • 49% say lack of biking tails and 27% say lack of public parks hinders physical activity • 94% acknowledged physical activity is key for disease prevention
What Makes the AFI Unique? • Many may ask, “Why do we need another study to tell us to get more active?” • Need an effective measure that captures: • The state of health • The state of community fitness • Measure at the local level • Scientific- and evidence-based measure
Advisory Board • Chair: Walter R. Thompson, Ph.D. FACSM(Georgia State University) • Vice-chair: Barbara Ainsworth, Ph.D. FASCM(Arizona State University) • Steven N. Blair, P.E.D., FACSM(University of South Carolina) • Ralph Bovard, M.D., MPH, FACSM(HealthPartners Specialty Center) • Jacqueline Epping, M.Ed.(U.S. Centers for Disease Control & Prevention) • John M. Jakicic, Ph.D., FACSM (University of Pittsburgh)
Advisory Board (cont’d) • Elizabeth Joy, M.D., MPH, FACSM(University of Utah) • NiCole Keith, Ph.D. FACSM (Indiana University Purdue University-Indianapolis) • Roseann M. Lyle, Ph.D. FACSM(Purdue University) • Melinda M. Manore, Ph.D, R.D., FACSM(Oregon State University) • Angela Smith, M.D., FACSM(Children’s Hospital of Philadelphia) • Stella Lucia Volpe, Ph.D., R.D. FACSM(University of Pennsylvania) • Wes Wong, M.D., M.M.M(Anthem Blue Cross Blue Shield-WellPoint)
AFI Program Goal • Improve the health, fitness and quality of life of Americans by promoting physical activity.
AFI Program Components • #1 - Data • Collect, aggregate and report metropolitan area data • Data related to: • Healthy lifestyles • Health outcomes • Community resources • Execute AFI data report • Scientific- and evidence-based snapshot of the health status of major metro areas
AFI Program Components • #2 - Resources • Resources for practical application of sports medicine and exercise science • Conduct research • Provide education
AFI Program Components • #3 - Health Promotion Partners • Link communities with organizations and existing programs in their metro area • Promote collaboration on physical activity and healthy lifestyle initiative • Connect local, state and national partners and resources
Implementation (Pilot) • Pilot phase focused on data collection and analysis (released May 2008) • Download at AmericanFitnessIndex.org • 16 of the most populous U.S. metro areas • Top 15 + Indianapolis • Based on MSA data from U.S. Census • Data collected, analyzed, weighted and aggregated
Implementation (Expansion) • The next phase focused on expanding the data report to the top 50 most populous U.S. metro areas • Download at AmericanFitnessIndex.org • Includes some newly available data
Methodology • AFI uses scientific evidence, expert opinion and statistical methodologies to select, weigh and combine the elements used in the data report.
Methodology • Metro Areas Included • Not city limits only • Overlooks interaction of core city and surrounding suburban areas • Shared fitness-related resources
Atlanta Austin Baltimore Birmingham Boston Buffalo Charlotte Chicago Cincinnati Cleveland Columbus, OH Dallas Denver Detroit Hartford Houston Indianapolis Jacksonville Kansas City Los Angeles Louisville Memphis Top 50 Metro Areas
Miami Milwaukee Minneapolis/St. Paul Nashville New York Oklahoma City Orlando Philadelphia Phoenix Pittsburgh Portland, OR Providence, RI Raleigh, NC Richmond, VA Riverside, CA Rochester, NY Sacremento St. Louis Salt Lake City San Antonio San Francisco San Jose Seattle Tampa Virginia Beach Washington, D.C. Top 50 Metro Areas
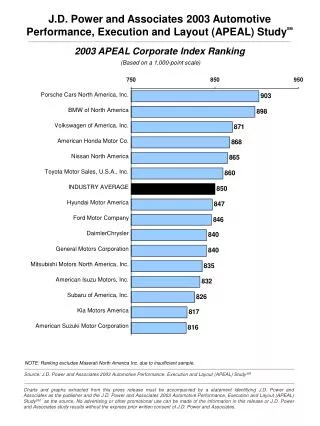
Metro Area Breakdown • Example: • Atlanta • AFI rank (5); AFI Score (285) • Population rank (9) • MSA: Atlanta-Sandy Springs-Marietta • Nickname: Metro Atlanta
Indicators Selected for AFI • Must be related to the level of health status and/or physical activity • Must be recently measured and reported by a well-respected agency or organization of the metro area • Must be modifiable through community efforts • Example: smoking rate
Data sources and information • Info gleaned from publicly available federal reports and past studies • Must be recent data with established history • Most data is from 2006
Data sources and information • SMART BRFSS • American Community Survey (by Trust for Public Land) • U.S. Census • U.S. Dept of Agriculture • State Report Cards • HRSA Area Resource File
Data on Personal Health • Health Behaviors • % exercising in last 30 days • % exercising at least moderately • % eating 5+ fruit/veggies per day • % currently smoking
Data on Personal Health • Chronic Health Problems • % obese • % in excellent or very good health • % with asthma • % with diabetes • Death rate/100,000 for CV disease • Death rate/100,000 for diabetes
Data on Personal Health • Health Care • % with health insurance
Data - Community/Environment • Built Environment • Parkland as % of MSA land area • Acres of parkland/1,000 • Farmers’ Markets/1,000,000 • #/10,000 using public transit to work • #/10,000 biking or walking to work
Data - Community/Environment • Recreational Facilities • Ball diamonds/10,000 • Dog parks/10,000 • Park playgrounds/10,000 • Golf courses/100,000 • Park units/10,000 • Recreation centers/20,000 • Swimming pools/100,000 • Tennis Courts/10,000
Data - Community/Environment • Park-related expenditures per capita • Level of State requirement for PE classes
Data - Health Care Providers • # of primary care providers/100,000
Data Limitations • Based on self-reported responses • Some missing data for some indicators in some MSAs • Example: Riverside community and environmental indicators
Guiding Principles for Healthy Communities • Overall health improvement in U.S. communities must focus on the prevention of behavioral-linked diseases by effectively addressing the underlying risk and community factors • The rise in chronic diseases attributable to physical inactivity and unhealthy diets are a “clear and present danger” to our health and healthcare systems, our communities, our nation and our future
Guiding Principles for Healthy Communities (cont’d) • All U.S. communities, irrespective of size and current health status, can make powerful advances in improving the health of their people through simple, affordable, effective steps. • There is a need for even more synergy and collaboration to assist U.S. communities in actively making the moves toward better health
Moving from pilot to full version • Expanded and enhanced • Expanded to the Top 50 MSAs • Use combined MSAs for communities with MSA divisions • Expand data elements from BRFSS • Obtain info about certified personal trainers • Update elements
Next Steps • May 2009 data report • Released during ACSM Annual Meeting (Seattle, Wash.) • Welcome suggestions and comments • Send comments to afi@acsm.org
What can you do? • Provide comments/suggestions • Be a role model for good health and physical activity • Educate and bring awareness to the physical inactivity epidemic in your community • Media relations • Engage community leaders • Volunteer • Check out www.americanfitnessindex.org for local resources
Thank you Questions? www.AmericanFitnessIndex.org