Download
1 / 30
390 likes | 714 Views
SMALLPOX AND CHICKENPOX. Dr Navya N Assistant professor Department of community medicine Yenepoya medical college. SPECIFIC LEARNING OBJECTIVES. At the end of the class the students should be able to Describe about eradication of smallpox

E N D
SMALLPOX AND CHICKENPOX DrNavyaN Assistant professor Department of community medicine Yenepoya medical college
SPECIFIC LEARNING OBJECTIVES • At the end of the class the students should be able to • Describe about eradication of smallpox • Explain the epidemiological determinants of chickenpox • Differentiate between the clinical features of chickenpox and smallpox • Describe about the preventive measures of chickenpox
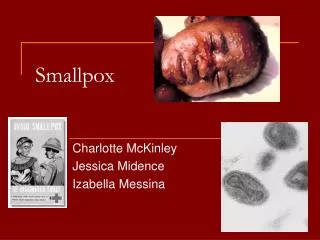
SMALLPOX • Acute infectious disease- Variola Virus • Clinically characterized- sudden onset of fever, headache, backache, vomiting sometimes convulsions- children. • Third day of fever- typical rash appears- centrifugal in distribution • Successive stages- macule papule, vesicle, pustule, and scab with subsequent scarring.
HISTORY • 1967- endemic in 33 countries • WHO – vast international campaign – 1967- 1979 – eradication • Last indigenous case in India- 17th may 1975 – Bihar • Last known case in India ( Importation –Bangladesh) – 24th may 1975 • April 1977 – India declared small pox free • Last case in the world – 26 october 1977 • Laboratory accident – 1978 • WHO Eradication of Small pox – 8th May 1980 • Vaccination – discontinued • WHO – reserve stock- vaccine and vaccination needles – emergency -200 million people
CASE DEFINITION – IHR ( 2005) • Member states – IHR (2005) – notify WHO immediately- any confirmed case Confirmed Case : • Individual- any age- acute fever ( >= 38.3o C / 101o F) , malaise, severe prostration with headache, backache- 2-4 days before- rash AND • Maculopapular rash – starting on face and forearms – trunk and legs • Within 48 hrs – deep seated, firm or hard , round well circumscribed vesicles – later pustules – umblicated or confluent AND • All lesions – same stage of development AND • No alternative diagnosis AND • Laboratory confirmation
EPIDEMIOLOGICAL FACTORS- ERADICATION • No known animal reservoir • No long term carrier of virus • Life long immunity- post recovery • Detection of cases – easy • Subclinical infection – did not transmit disease • Animal reservoir- absent • Vaccine – highly effective, easily administered , heat stable, long term protection • International cooperation
Eradication – everted – 2 million deaths, - few hundred thousand cases – blindness 10-15 million cases of disease / year- prevented • Smallpox virus- not completely destroyed stocks – govt research centres – US and Russian Federation
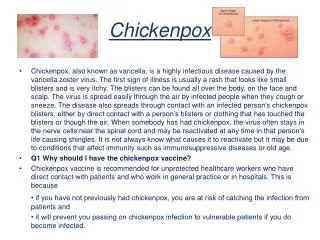
CHICKENPOX • Chickenpox/ varicella- acute, highly infectious disease- varicella-zoster (V -Z) virus. • Characterized- vesicular rash- accompanied by fever and malaise • Epidemic and endemic forms • Chickenpox and herpes zoster- different host responses- same aetiological agent. • Inoculation of zoster vesicle fluid into children produces chickenpox • Children- recovered from zoster virus related infection- resistant to varicella
PROBLEM STATEMENT • Global annual chickenpox disease burden – 4.2 million severe complications 4,200 deaths • Pre vaccine era – case fatality rate - developed countries – 3/lac cases compared to 1-3/ 1000 cases for measles • Factors – influence – severity and outcome : • proportion of cases- infants, pregnant women, other adults , • prevalence – immunocompromised conditions , • extent of access to care and appropriate treatment INDIA : • 2013 - 28,090 cases with 61 deaths • Case fatality rate – 0.21% • Highest cases- Kerala • Highest deaths – West Bengal
EPIDEMIOLOGICAL DETERMINANTS – AGENT FACTORS (a) AGENT : V-Z virus is also called "Human (alpha) herpes virus 3". • Primary infection causes chickenpox. • Recovery from primary infection- followed- establishment- latent infection- cranial nerves sensory ganglia and spinal dorsal root ganglia- without clinical manifestations. • Cell-mediated immunity wanes with age or following immuno-suppressive therapy- virus may reactivate- herpes zoster- 10-30%. • Herpes zoster - Painful. vesicular, pustular eruption in the distribution of one or more sensory nerve roots.
EPIDEMIOLOGICAL DETERMINANTS – AGENT FACTORS (b) SOURCE OF INFECTION: case of chickenpox, rarely – patient with herpes zoster • Virus- oropharyngeal secretions and lesions- skin and mucosa. • Virus- readily isolated- vesicular fluid during the first 3 days of illness. • Scabs- not infective
EPIDEMIOLOGICAL DETERMINANTS – AGENT FACTORS (c) INFECTIVITY: • Period of communicability-1 to 2 days before appearance of rash, 4 to 5 days thereafter • Virus tends to die out before pustular stage • Patient ceases to be infectious- lesions have crusted (d) SECONDARY ATTACK RATE: Secondary attack rate- household contacts- 90%
EPIDEMIOLOGICAL DETERMINANTS – HOST FACTORS • AGE : Primarily- children under 10 years of age. • Disease- severe- normal adults. • IMMUNITY : One attack- durable immunity; second attacks- rare. • Maternal antibody protects- infant- first few months of life. • No age- exempt in- absence of immunity. • IgG antibodies persist for life and their presence- protection against varicella. • Cell-mediated immunity- important in recovery from V-Z infections and protection against- reactivation • PREGNANCY : Presents a risk - foetus and the neonate
EPIDEMIOLOGICAL DETERMINANTS – Environmental factors Environmental factors : seasonal trend in India- mostly- first six months of the year. • Over-crowding favours- transmission. Transmission : person to person- droplet infection and by droplet nuclei. • Most patients- infected- "face-to-face" (personal) contact. • Portal of entry- respiratory tract. • Virus extremely labile- unlikely- fomites • Contact infection- individual- herpes zoster- index case. • Virus - cross the placental barrier and infect the foetus- congenital varicella.
Clinical features • Incubation period- 14 to 16 days, • Clinical spectrum of chickenpox- mild illness- few scattered lesions- severe febrile illness- widespread rash. • Inapparent infection- no more than 5 per cent- susceptible children • Majority- disease- mild and typical • Two stages : • Pre eruptive stage • Eruptive stage
Clinical features -PRE-ERUPTIVE STAGE : • Onset- sudden • Mild- moderate fever • Pain in the back, • Shivering and malaise. • This stage- very brief- lasting about 24 hours. • In adults- prodromal- more severe- last for 2-3 days before rash
Clinical features -ERUPTIVE STAGE : • Children- rash- often first sign- comes- day the fever starts. • Distinctive features- rash are : • Distribution : symmetrical. • First appears- trunk- abundant, and then comes on the face, arms and legs- less abundant. • Mucosal surfaces (e.g., buccal, pharyngeal)- generally involved. • Axilla- affected, but palms and soles- not usually affected. • Density of eruption diminishes centrifugally.
Clinical features -ERUPTIVE STAGE 2. Rapid evolution : • Rash advances quickly- macule papule vesicle scab. • First to attract attention- vesicles filled with clear fluid- "dew-drops" on the skin. • Superficial in site- easily ruptured walls and surrounded- area of inflammation. • Not umbilicated. • Vesicles- form crusts without going through- pustular stage. • Scabbing begins 4- 7 days after- rash appears.
Clinical features -ERUPTIVE STAGE 3. Pleomorphism :characteristic feature- all stages of rash(papules, vesicles and crusts)- seen simultaneously at one time- same area. • Rash appears- successive crops- 4 to 5 days- same area. 4. Fever: Not high, but - exacerbations with each fresh crop of eruption.
COMPLICATIONS • Mortality- < 1%- uncomplicated cases. • Complications- immunosuppressed/ normal children and adults. • Haemorrhages (varicella haemorrhagical), • Pneumonia - neonates, adults and immuno-compromised patients- varicella related deaths • Encephalitis • Acute cerebeller ataxia • Reye's syndrome (acute encephalopathy associated with fatty degeneration- viscera especially liver)
COMPLICATIONS • Maternal varicella- foetal wastage and birth defect, low birth weight, cataract, microphthalmia, chorioretinitis, deafness and cerebro-cortical atrophy. • Varicella- mother within 5 days after delivery, the newborn risk-disseminated disease • Secondary bacterial infections- group A beta haemolytic streptococci and staphylococcus aureus • Cellulitis, erysipelas, epiglottitis, osteomyelitis, scarlet fever, rarely meningitis. • Pitted scars- frequent sequelae. • lmmunocompromised patients- Disseminated intravascular coagulation • Children with leukaemia- prone to severe disseminated varicella-zoster virus disease
LABORATORY DIAGNOSIS • Laboratory diagnosis is rarely required, clinical signs- usually clear-cut. • The most rapid and sensitive- vesicle fluid- electronic microscope. CONTROL : • Notifications, • Isolation of cases - 6 days after onset of rash • Disinfection of articles soiled by nose and throat discharges • Several antiviral compounds- effective therapy • Acyclovir, valacylovir, famiciclovir and foscarnet
SUMMARY • WHO eradication of smallpox – 8th may 1980 • Small pox vaccine – discontinued • Chicken pox – varicella zoster virus • Highly infectious – Respiratory route • Characteristic features – rashes abundant in trunk and back, rapid evolution, pleomorphism • Complications of chickenpox – most commonly – adults and immunocompromised • Pneumonia – most common complication leading to varicella related deaths • Vaccination