Download
1 / 30
310 likes | 537 Views
LEUKEMIAS Dr Mehboob Khan Pathologist. Leukemias are malignancies of hemtopoietic cells or tissues in which there is abnormal proliferation of hemopoietic cells with infiltration of bone marrow and lymphatic tissues ETIOLOGY: Molecular biology of leukemogenesis - oncogenes

E N D
Leukemias are malignancies of hemtopoietic cells or tissues in which there is abnormal proliferation of hemopoietic cells with infiltration of bone marrow and lymphatic tissues ETIOLOGY: • Molecular biology of leukemogenesis- oncogenes • Abnormalities of the chromosomes- translocation deletions • Radiation • Chemicals • Viruses • Genetic factors-Down syndrome
CLASSIFICATION • LYMPHOID • ACUTE LYMPHOID LEUKEMIA (ALL) • CHRONIC LYMPHOID LEUKEMIA (CLL) • MYELOID • ACUTE MYELOID LEUKEMIA (AML) • CHRONIC MYELOID LEUKEMIA (CML)
ACUTE MYELOID LEUKEMIA
AML -NOT OTHERWISE CLASSIFIED MORPHOLOGIC CLASSIFICATION
MYELOBLAST WITH AUER ROD
NORMOBLASTS MYELOBLAST
AML-M4 AML-M5 AML-M6 MEGAKARYOBLASTS
CLINICAL FEATURES OF ACUTE LEUKEMIA: • COMMON • Anemia • Fever • Malaise • Hemorrhages, bruising and petechiae • LESS COMMON: • Infections of mouth and pharynx • Pains in bones and joints • URTI (children) • Superficial lymph node enlargement (children in ALL) • OCCASIONAL: • Abdominal pain • Skin rashes • Gum hypertrophy • Mediastinal obstruction
CLINICAL FEATURES DUE TO ORGAN INFILTRATION: • Tender bones • Superficial lymphadenopathy (ALL) • Splenomegaly, hepatomegaly (ALL) • Gum hypertrophy and infiltration, rectal ulceration and skin involvement (AML- myelomonocytic and andmonocytic type) • Meningeal syndrome (ALL) • Testicular swelling and mediastinal compression (ALL)
BLOOD PICTURE: • Normocytic and normochromicanemia • Total WBC count may be increased upto 500 x 10 /L • Thrombocytopenia • Peripheral blood smear- myeloblasts, promyelocytes, myelocytes , metamyelocytes, agranular neutrophils, stab cells, myelomonocytes and normoblasts • Bone marrow- hypercellular with plenty of blast cells (>75% of the marrow cell population) THERE SHOULD BE AT LEAST 30% BLASTS IN BONE MARROW (FAB ) 20% BLASTS IN BONE MARROW (WHO) 6. Tests for DIC will be positive in Promyelocyticleukemia
3. CYTOCHEMISTRY • Myeloperoxidase- positive in immuture myeloid cells containing granules and auer rods but negative in M0 myeloblasts • Sudan black- positive in immature cells in AML • Non specific esterase (NSE)- positive in monocytic series (M4 and M5) • Periodic acid Schiff (PAS)- positive in immature lymphoid cells and in erythroleukaemia (M6) • Acid phosphatase – focal positive in leukaemic blasts in ALL and diffuse reaction in monocytic cells (M4 and M5)
MYELOBLAST (MYELOPEROXIDASE POSITIVE)
4. IMMUNOPHENOTYPING • AML cells express CD13 and CD33 antigens • M5 shows CD41 and CD42 positivity • ALL is positive for CD10, CD19 in Pre B ALL (90%); B cell ALL (50%); • ALL T cell type are positive for CD1,CD2, CD5, CD7 5. OTHER INVESTIGATIONS • Serum muramidase- elevated in M4 and M5 AML • Serum uric acid- frequently elevated
COURSE AND PROGNOSIS IN AML: • GOOD PROGNOSIS • Age <40 year • M2,M3 and M4 types • Blast cells with Auer rods • Total WBC <25,000/cumm • Tranlocation and inversion • Leukemia without preceding Myelodysplastic syndrome (MDS) • BAD PROGNOSIS: • Age<2 years and >55 years • M0,M6,M7 types • Total WBC >100,000/cumm • Deletions • Leukemia with preceding MDS
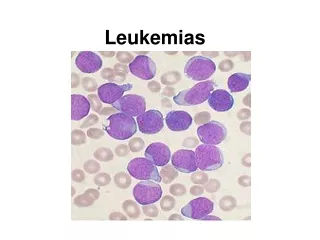
ALL is the commonest leukemia seen in childhood • The predominant cell seen in ALL is LYMPHOBLAST • Lymphoblast has coarse nuclear chromatin and 1-2 nucleoli, high nucleus:cytoplasmic ratio (N:C), stain positve for PAS (periodic acid Schiff) and TdT (terminal deoxynucleotidyltransferase)
LYMPHOBLASTS (ALL)
MYELOBLASTS LYMPHOBLASTS
FAB CLASSIFICATION OF ALL • L1 ALL • Commonest type • Best prognosis • Lymphoblasts have coarse chromatin with small nucleoli and scanty cytoplasm • L2 ALL • Lymphoblasts have heterogenous chromatin with 1-2 nucleoli, moderate cytoplasm with few vacuoles • L3 ALL • Rare and worst prognosis • Homogenous chromatin with 1-2 prominent nucleoli, abundant cytoplasm and vacolues positive for Oil O Red
WHO IMMUNOLOGICAL CLASSIFICATION OF ALL • B CELL • More common • CD19 and Cd20 positive • Associated with pancytopenia • T CELL • Less common • CD1, CD2, CD7 positive • Associated with mediastinal mass, lympadenopathy and splenomegaly
CLINICAL FEATURES: • Same as AML • With lymphadenopathy, hepatsplenomegaly BLOOD PICTURE: • Elevated total WBC count upto 500,000/cum • Anemia, neutropenia • Thrombocytopenia • Lymphoblasts >30% in bone marrow BIOCHEMICAL CHANGES: • Elevated uric acid, LDH levels • Elevated serum phosphate levels • Hypocalcemia
PROGNOSIS IN ALL GOOD PROGNOSIS • Age 2-8 years • Females • L1 type • Pre-B cell • Absence of mediastinal mass • Hyperdiploidy or translocations BAD PROGNOSIS • Age < 2 year , >10 years • Male • L2 and L3 type • Pre T cell • Mediastinal mass • Ph chromosome