Download
1 / 65
730 likes | 1.39k Views
Drugs Used for Treatment of Osteoporosis and Rickets/ Osteomalacia. Dr. Kaukab Azim. MBBS, PhD. What is Osteoporosis.

E N D
Drugs Used for Treatment of Osteoporosis and Rickets/Osteomalacia Dr. Kaukab Azim. MBBS, PhD
What is Osteoporosis “a disease characterized by low bone mass and microarchitectural deterioration of bone tissue, leading to enhanced bone fragility and a consequent increase in fracture risk.”
Incidence of osteopenia and osteoporosis This data is for US. (William’s textbook of Endocrinology)
Normal Calcium Turnover Diet 1000 mg 300 mg 175 mg 500 mg Gut Gut Bone Bone ECF Ca++ 900 mg 125 mg 500 mg 9825 mg Reabsorbed 10,000 mg Filtered / day Feces 825 mg Urine Kidney 175 mg Greenspan’s. Basic and Clinical Endocrinology
Bisphosphonates Bisphosphonates are agents that prevent the breakdown of bone. PROTOTYPES AND COMMON DRUGS Aminobisphosphonates • Prototype: alendronate • Others: risedronate,pamidronate Non-Aminobisphosphonates • Prototype: etidronate • Others: clodronate,tiludronate,zoledronate
Mechanism of Action • The structural integrity of bone is determined to a large extent by the balance between the activity of osteoclasts, which break down bone (resorptive), and the activity of osteoblasts, which build bone. • Bisphosphonates (BPs) inhibit osteoclast activity through a variety of mechanisms, some better understood than others. • Inside the osteoclast the aminobisphosphonates disrupt the mevalonatepathway. Disruption of the mevalonate pathway interrupts osteoclast function and leads to apoptosis of the osteoclast.
The non-aminobisphosphonateswork by increasing the accumulation of cytotoxic metabolites within osteoclasts, interfering with their function and possibly leading to osteoclast cell death. • The clawlike chemical structure of BPs facilitates their attachment to bone. The BPs remain within the matrix until the acids released by the osteoclasts break down the matrix and liberate the BPs. The activity of osteoclasts results in their own death. • Osteoclasts die after ingesting BP molecules. • BPs also inhibit vitamin D production, intestinal Ca2+ transport, and cell growth.
Pharmacokinetics • BPs have very low oral bioavailability (<10%), and their absorption is further reduced by food and by divalent cations such as calcium. It is therefore recommended that BPs be taken on an empty stomach, with plain water. • The BPs that are absorbed are highly bound to bone, and are not metabolized, nor do they inhibit or induce metabolizing enzymes. They are eliminated by the kidney. • The oral BPs are typically administered once daily. A higher dose of alendronate is also available as a once weekly formulation.
Indications • Osteoporosis • Paget's disease of the bone (results in enlarged, deformed bones) • Hypercalcemia: ▴ Malignancy ▴ Primary hyperparathyroidism (continuous parathyroid hormone [PTH] release causes bone demineralization) • Bone metastasis causing osteolysis: ▴ Multiple myeloma ▴ Bone metastases of malignant tumors
Contraindications • Hypocalcemia: BPs have exhibited decreases in serum calcium, so it is recommended that any deficiencies in calcium be addressed before initiation of therapy. • Poor renal function: BPs are eliminated renally, so patients with creatinine clearance <30 mL/min may experience accumulation of these agents.
Side Effects • Gastrointestinal:nausea, dyspepsia Serious • Esophagitis or esophageal erosion • Osteonecrosis of the jaw Aminobisphosphonates • Fever, flulike symptoms
Parathyroid hormone TERIPARATIDE This is a recombinant form of naturally occurring PTH.
Mechanism of Action • PTH is released from the parathyroid gland. It regulates calcium and phosphate flux across cell membranes in bone and kidney. The key effects of PTH are as follows: Increased serum calcium Decreased serum phosphate Increased osteoclast activity in bone • The effects on osteoclasts are indirect. PTH increases activity of the RANK (receptor activator of nuclear factor κ) ligand (RANKL). RANKL regulates osteoclast activity • PTH increases both bone resorption and formation. High levels of PTH increase bone resorption
Low levels of intermittent PTH, however, can enhance bone formation. The anabolic actions of PTH are mediated through the PTH-1 receptors on osteoblasts. PTH also stimulates insulin-like growth factor (IGF-1) in osteoblasts, and IGF-1 also has anabolic effects on bone. • It is still not clear why high, sustained PTH has a catabolic effect, whereas low, intermittent administration has an anabolic effect on bone.
In addition to these factors, PTH has several effects on the kidney: Increased reabsorption of Ca2+ and Mg2+ Decreased reabsorption of phosphate, amino acids, bicarbonate, Na+, Cl-, and sulfate Stimulation of production of 1,25 dihydroxyvitamin D
Pharmacokinetics • Teriparatideis administered as a subcutaneous injection once daily. • It is both rapidly absorbed and rapidly eliminated, with plasma concentrations reaching their peak at 30 minutes post-injection and falling to undetectable levels after 3 hours. • The metabolism of teriparatide is poorly understood, but enzymes are thought to be involved.
Indications • Osteoporosis Typically reserved for severe osteoporosis and/or patients in whom previous therapies, including the BPs, have failed • Osteoporosis secondary to corticosteroid use
Contraindications • Children or young adults with open epiphysis • Hypercalcemia • Active Paget's disease of bone. • Skeletal metastases or skeletal malignant conditions: risk of osteosarcoma • History of radiation to the skeleton: risk of osteosarcoma. • Pregnancy and lactation
Side Effects • Hypercalcemia(mild):This can be managed by reducing Ca2+ and vitamin D intake or by adjusting teriparatide dose from daily to every other day. • Leg cramps(may occur) • Nausea(may occur) • Orthostatic hypotension
Estrogens • The decline in estrogen levels is a major factor in postmenopausal osteoporosis, and there is evidence that giving hormone replacement therapy (HRT) can ameliorate this condition. But HRT has actions on many systems • The prevailing hypothesis advanced to explain these observations is that estrogens reduce the bone-resorbing action of PTH. Estrogen administration leads to an increased Vit D level in blood. The increased Vit D levels may result from decreased serum calcium and phosphate and increased PTH.
Estrogen receptors have been found in bone in both males and females, and estrogen has direct effects on bone remodeling. Men who lack the estrogen receptor have marked osteopenia. This further substantiates the role of estrogen in bone development, even in men. • The principal therapeutic application for estrogen administration in disorders of bone mineral homeostasis is the treatment or prevention of postmenopausal osteoporosis.
Adverse Effects of Estrogens • Migraine headaches • Waterretention(weight gain) • Stimulation of reproductive organ tissues: Vaginal bleeding or spotting (because of growth of endometrial tissue) Enlargedfibroids Breast tenderness • Gall bladder disease (primarily stones) • Thrombosis: (estrogen is a procoagulant) Deep vein thrombosis and pulmonary embolism Stroke Coronary heart disease • Increased triglycerides
Raloxifene Many women fear adverse effects of estrogen therapy, particularly the increased risk of breast cancer from continued estrogen use (the well-demonstrated increased risk of endometrial cancer is prevented by cycling with a progestin) and do not like the persistence of menstrual bleeding that often accompanies this form of therapy. Raloxifene. Selective Estrogen Receptor Modulator (SERM) Reloxifene shares some of the beneficial effects of estrogen on bone without increasing the risk of breast or endometrial cancer (it may actually reduce the risk of breast cancer). Although not as effective as estrogen in increasing bone density, raloxifene has been shown to reduce vertebral fractures.
Mechanism of Action Actions and mechanism of action • Raloxifene produces a dose-dependent increase in osteoblast activity and reduction in osteoclast action. Pharmacokinetics • It is well absorbed in the gastrointestinal tract, and undergoes extensive first-pass metabolism in the liver. (Colestyramine, given with it, reduces the enterohepatic cycling of raloxifene by 60%.) • Thus bioavailability is only about 2%. It is widely distributed in the tissues, and is converted to an active metabolite in liver, lungs, bone, spleen, uterus and kidneys. Its half-life averages 32 hours. It is excreted mainly in the faeces.
Unwanted effects • Hot flushes and leg cramps are common. In a recent clinical trial, raloxifene was found to be associated with venous thromboembolism; however, other authorities state that there is less risk of this adverse effect in younger patients.
Strontium Reanelate This compound, newly introduced for treatment of osteoporosis, is composed of two atoms of strontium combined with organicranelic acid. It inhibits bone resorption and also stimulates bone formation. Mechanism of Action Strontium is similar to calcium as regards its absorption in the gastrointestinal tract, its incorporation into bone and its renal elimination. Strontium atoms are exchange for calcium in the bone minerals and remain in the bone for many years. Pharmacokinetics The drug is well tolerated; a low incidence of nausea and diarrhoea is reported.
Calcitonin The main preparation available for clinical use is salcatonin(synthetic salmon calcitonin). Synthetic human calcitonin is now also available. Calcitonin is given by subcutaneous or intramuscular injection, and there may be a local inflammatory action at the injection site. It can also be given intranasally. Its plasma half-life is 4-12 minutes, but its action lasts for several hours. Adverse effects include nausea and vomiting, facial flushing, tingling sensation in the hands and an unpleasant taste in the mouth.
Osteomalacia and Rickets Osteomalacia(referred to as rickets in children) is defined as an excess organic bone matrix secondary to defective or inadequate bone mineralization Predominantage: Allages.It is usually a disease of the older population (50-80). Predominant sex: Female > Male (slightly)
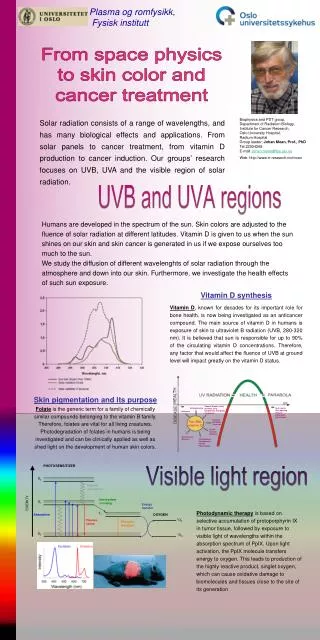
Vitamin D synthesis and activation Vitamin D is synthesized in the skin in response to ultraviolet radiation and is also absorbed from the diet. It is then transported to the liver, where it undergoes 25-hydroxylation. This metabolite is the major circulating form of vitamin D. The final step in hormone activation, 1-hydroxylation, occurs in the kidney.
Rickets and Osteomalacia Rickets • In children, prior to epiphyseal fusion, vitamin D deficiency results in growth retardation associated with an expansion of the growth plate known as rickets. Osteomalacia • In adults the hypocalcemia and hypophosphatemia that accompany vitamin D deficiency result in impaired mineralization of bone matrix proteins, a condition known as osteomalacia.
Causes • Vitamin D deficiency (most common)caused by reduced exposure to sunlight, poor nutrition, malabsorptionsyndromes. • Defective metabolism of parent vitamin D to active metabolites • Drug-induced, i.e., anticonvulsants – phenytoin, chronic renal failure, hypophosphatemia, long-termhemodialysis RISK FACTORS • Poverty • Inadequate nutrition and sunlight exposure