Download
1 / 40
410 likes | 538 Views
Central Nervous System ( CNS ) . Done by the group of CNS For ABC medicine, for year 2013 Faculty of medicine, UQU, Makkah , K.S.A. Objectives : . By the end of this show you should : Have the approach to get the Dx . Be able to know how to take a good neurological Hx .

E N D
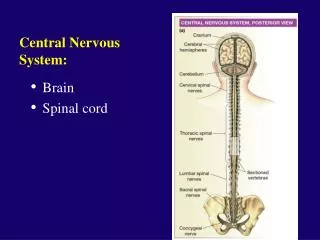
Central Nervous System ( CNS ) Done by the group of CNS For ABC medicine, for year 2013 Faculty of medicine, UQU, Makkah, K.S.A
Objectives : By the end of this show you should : • Have the approach to get the Dx. • Be able to know how to take a good neurological Hx. • Be able to do the neurological examinations with proper technique. • Do a 3 min.s CNS examination. • Know some important neurological diseases. • Know & memorize some specific terms in neurology.
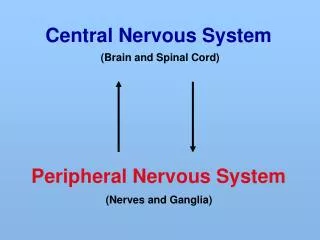
The approach • History ( Hx ). • Physical examination. • Investigation ( Ix ). • Differential diagnosis ( DDx ).
Q : How to approach the history taking? • Establish a good relationship. • Listen carefully. • Interrupt appropriately. • Note non-verbal clues. • Correctly interpret the information.
Hx • ID : • Name, age, sex, nationality, admit through? and time of admission. • Chief complaint : • Presenting symptoms and duration.
Presenting symptoms in CNS • Headache. • Facial pain. • Neck or back pain. • Fits. • Loss of consciousness. • Syncope, dizziness or vertigo. • Disturbances of vision, hearing, smell or speech. • Loss of or disturbed sensation. • Weakness in limbs. • Involuntary movements or tremor. • Disturbances of sphincter control.
Hx • History of presenting illness ( HPI ) : • Details of current illnesses : • Duration. • Onset ( acute, subacute or chronic ). • Course of the condition ( static, progressive, or relapsing and remitting ). • Severity ( Estimate functional limitation ). • Site ( e.g. headache ). • Radiation. • Nature. • Aggravating and reliving factors. • Diurnal or seasonal variation. • Associated symptoms. • Risk factors. • Previous episodes and current treatment. • Review of CNS.
Hx • Past history : • Medical illnesses. • Surgical operations. • Past or current treatment (name and dosage). • Allergies (food, drugs or animals). • Blood transfusion. • Family history : • Similar illnesses. • Chronic diseases ( HTN, DM, IHD … etc ).
The Hx • Social history : • Occupation. • Education. • Marital status. • Smoking. • Alcohol. • Travel Hx. • Living conditions. • Systemic review : ( 7 systems without the CNS )
Risk factors of cerebrovascular disease • HTN • Smoking • DM • Hyperlipidemia • Atrial fibrillation ( emboli ) • Hematological disease • Family Hx of stroke
Q : How to approach the physical exam? • Introduction : ( always keep the 9 of them in mind ) • Chaperon if female patient ( pt ). • Introduce yourself and build a good relationship with the pt. • Take permission. • Secure the privacy of the pt. • Wash your hands. • Stand in the right ( Rt. ) side of the pt. • Put the pt. in the proper posture. • Make a proper exposure. • Explain what you will do before examining the pt. • ALWAYSstart byABCDE(F/V) i.e. Appearance, Bodybuild, Connection, Disability or Deformity, Environmentaroundthepatient, and then the Vitals. • The vitals are( PORT-B ) i.e. Pulse, Oxygensaturation, Respiratoryrate, TemperatureandBlood pressure. • ALWAYSstart by general then go specific. • ALWAYSstart by Inspection then Palpation then Percussion then Auscultation.
After the introduction and doing the ABCD and after checking the vitals, we’ll start our neurological examination by : • Assessment of the higher centers and speech : I. Handedness. By asking the pt. if he/she is Rt. or Lt. handed to assess the likely dominant hemisphere. II. Orientation ( person names, place and time ). The disorientation may be acute and reversible i.e. delirium, or chronic and irreversible as in dementia. III. Speech. Ask the pt. to speak freely or ask him/her to describe the room and …. etc to see if there were any speech problem e.g. dysarthria, dysphonia or dysphasia. • Abnormal movements. Just by observation check if there were any obvious tremors, tics … etc
2. Cranial Nerves ( CN ) : As you know the CNs has either pure sensory or pure motor or mixed component, in the following table you’ll find brief information about each CN.
Q : How to examine the CNs? • Inspection. • Palpation : • Sensory. • Motor. • Reflexes.
We’ll focus only in what could come in the OSCE exam, starting with : • CN II : • Visual Acuity. Test visual acuity for each eye separately ( by covering one eye at a time ) using an eye chart. • Visual Fields. Test visual fields for each eye by asking the patient to fixate straight ahead and to report when a finger can be seen moving in each quadrant. Alternatively, ask the patient to report how many fingers are being shown in each quadrant
CN III, IV, VI : • First, record the pupil size and shape at rest. • Pupil Light Reflex. • note the direct response, meaning constriction of the illuminated pupil, as well as the consensual response, meaning constriction of the opposite pupil. • Swinging Flashlight. • In an afferent pupillary defect there is a decreased direct response caused by decreased visual function in one eye. This can be demonstrated with the swinging flashlight test, in which the light is moved back and forth between the eyes every two to three seconds. The afferent pupillary defect becomes obvious when the flashlight is moved from the normal to the affected eye, and the affected pupil dilates in response to light. • Accommodation. • Normally, the pupils constrict while fixating on an object being moved from far away to near the eyes. • Eye movements. • Check extraocular movements (eye movements) by having the patient look in all directions without moving their head and ask them if they experiences any double vision or if you notice a nystigmus.
Q : What is Being Tested? • Direct response ( pupil illuminated ). The direct response is impaired in lesions of the ipsilateral optic nerve, the pretectalarea, the ipsilateralparasympathetics traveling in CN III, or the pupillary constrictor muscle of the iris. • Consensual response ( contralateral pupil illuminated ). The consensual response is impaired in lesions of the contralateral optic nerve, the pretectal area, the ipsilateralparasympathetics traveling in CN III, or the pupillary constrictor muscle. • Accommodation ( response to looking at something moving toward the eye ). Accommodation is impaired in lesions of the ipsilateral optic nerve, the ipsilateralparasympathetics traveling in CN III, or the pupillary constrictor muscle, or in bilateral lesions of the pathways from the optic tracts to the visual cortex. Accommodation is spared in lesions of the pretectal area.
CN V : • Sensory : • Facial Sensation. Test facial sensation using a cotton wisp and a sharp object. • Motor: • Muscles of mastication i.e. Temporal and masseter muscles Ask the pt. to clench the teeth then inspect for wasting of masseter and temporal muscles. • Reflexes : • Corneal Reflex. It is tested by touching each cornea gently with a cotton wisp and observing any asymmetries in the blink response. • Jaw jerk reflex. by gently tapping on the jaw with the mouth slightly open, if present, it mean hyper-reflexia which is abnormal.
CN VII : • Motor : • Muscles of Facial Expression. Look for asymmetry in facial shape or in depth of furrows such as the nasolabial fold. Also look for asymmetries in spontaneous facial expressions and blinking. Ask patient to smile, puff out their cheeks, clench their eyes tight, wrinkle their brow, and so on. • Sensory : • Taste sensation from anterior 2/3 of the tongue. Check taste with sugar, salt, or lemon juice on cotton swabs applied to the lateral aspect of each side of the tongue. Like olfaction, taste is often tested only when specific pathology is suspected, such as in lesions of the facial nerve.
Q : What is Being Tested? • Facial weakness can be caused by lesions of upper motor neurons in the contralateral motor cortex or descending central nervous system pathways, lower motor neurons in the ipsilateral facial nerve nucleus ( CN VII ) or exiting nerve fibers, the neuromuscular junction, or the face muscles. • Note that the upper motor neurons for the upper face ( the upper portions of the orbicularisoculi and the frontalis muscles of the forehead ) project to the facial nuclei bilaterally. • Therefore, upper motor neuron lesions, such as a stroke, cause contralateral face weakness sparing the forehead, while lower motor neuron lesions, such as a facial nerve injury, typically cause weakness involving the whole ipsilateral face.
CN IX, X : • Palate Elevation. • Does the palate elevate symmetrically when the patient says, "Aah"? • Gag Reflex. • Does the patient gag when the posterior pharynx is brushed? The gag reflex needs to be tested only in patients with suspected brainstem pathology, impaired consciousness, or impaired swallowing. • CN XI : • Sternocleidomastoid and Trapezius Muscles. • Ask the patient to shrug their shoulders, turn their head in both directions, and raise their head from the bed, flexing forward against the force of your hands.
CN XII : • Tongue Muscles. • Note any atrophy or fasciculations (spontaneous quivering movements caused by firing of muscle motor units) of the tongue while it is resting on the floor of the mouth. • Ask the patient to stick their tongue straight out and note whether it curves to one side or the other. • Ask the patient to move their tongue from side to side and push it forcefully against the inside of each cheek. • Fasciculations and atrophy are signs of lower motor neuron lesions. Unilateral tongue weakness causes the tongue to deviate toward the weak side. Tongue weakness can result from lesions of the tongue muscles, the neuromuscular junction, the lower motor neurons of the hypoglossal nerve (CN XII), or the upper motor neurons originating in the motor cortex. Lesions of the motor cortex cause contralateral tongue weakness.
3. Motor system examination : • Upper & Lower limbs. • Inspection : you should comment on all the following : • Posture of the limb, any deformity, obvious muscle wasting, atrophy, involuntary movements, lesions or scars, fasciculation, arm drifting and neurocutanous manifestations . • Palpation : • Muscle measurement. • Fasciculation. • Tone : • Ask the patient to relax, and then passively move each limb at several joints to get a feeling for any spastic resistance or rigidity that may be abnormally present. • Check also for clonus in the ankle and the knee “ pateller “.
Power : • Test the strength of each muscle group and record it in a systematic fashion. • It is wise to pair the testing of each muscle group immediately with testing of its contralateral counterpart to enhance detection of any asymmetries. • Muscle strength is often rated on a scale of 0/5 to 5/5 as follows : • 0/5 : no contraction. • 1/5 : muscle flicker, but no movement. • 2/5 : movement possible, but not against gravity ( test the joint in its horizontal plane ). • 3/5 : movement possible against gravity, but not against resistance by the examiner • 4/5 : movement possible against some resistance by the examiner ( sometimes this category is subdivided further into 4–/5, 4/5, and 4+/5 ). • 5/5 : normal strength. • While testing muscle strength, it is important to keep in mind anatomic information such as which nerves, nerve roots, and brain areas control each muscle and to allow this information to guide the exam. • Also compare proximal versus distal weakness because these features can sometimes suggest muscle versus nerve disease, respectively.
Reflexes : • Check the deep tendon reflexes using impulses from a reflex hammer to stretch the muscle and tendon. The limbs should be in a relaxed and symmetric position, since these factors can influence reflex amplitude. • Compare each reflex immediately with its contralateral counterpart so that any asymmetries can be detected. • Deep tendon reflexes are often rated according to the following scale : • 0 : absent reflex • 1+ : trace, or seen only with reinforcement • 2+ : normal • 3+ : brisk • 4+ : nonsustainedclonus (i.e., repetitive vibratory movements) • 5+ : sustained clonus. • Check also the planter reflex for +veBabiniski sign.
4. Sensory system examination • Self reading, read the Technique from the book or the website.
5. Co-ordination. • Upper limb : • Finger-nose test. • in which the patient is asked to alternately touch their nose and the examiner's finger as quickly as possible • Rapid alternating movement. • such as wiping one palm alternately with the palm and dorsum of the other hand • Rebound test. • Arm drifting. • by having the patient hold up both arms or both legs and close their eyes. • Lower limb : • Heel-shine test. • the patient is asked to touch the heel of one foot to the opposite knee and then to drag their heel in a straight line all the way down the front of their shin and back up again. • Toe-finger test. • Foot tapping test. • rapid foot tapping against the floor or other object.
6. Gate : • Go and turn around quickly, then walk back. • Draw a line in the floor. Then ask the pt. to walk on it. • Walk heel-to-toe. • Walk on toes. • Walk on heels. • Squat then stand up. • Romberg test. • Ask the patient to stand with their feet together (touching each other). Then ask the patient to close their eyes. • Remain close at hand in case the patient begins to sway or fall.
Q : What is Being examined Romberg test? • With the eyes open, three sensory systems provide input to the cerebellum to maintain truncal stability. These are vision, proprioception, and vestibular sense. If there is a mild lesion in the vestibular or proprioception systems, the patient is usually able to compensate with the eyes open. When the patient closes their eyes, however, visual input is removed and instability can be brought out. • If there is a more severe proprioceptive or vestibular lesion, or if there is a midline cerebellar lesion causing truncal instability, the patient will be unable to maintain this position even with their eyes open. • Note that instability can also be seen with lesions in other parts of the nervous system such as the upper or lower motor neurons or the basal ganglia, so these should be tested for separately in other parts of the exam.
Some important neurological conditions A. Meningeal irritation : • Neck Stiffness : first ask the pt. to flex his/her neck passively, then do it yourself actively. • Kernig sign : flex the hip fully & then try to extend the knee slowly +ve ( if there is resistance or pain in neck or back ). • Brudzinski sign : flex the neck while observing the hip & the knee +ve ( if there is hip &knee flexion with back pain ). • The UMNL & LMNL :
Facial palsy. • Known also as Bell’s palsy. • It is a unilateral facial paralysis of sudden onset due to a lesion of the facial nerve, resulting in characteristic facial distortion. • Causes : ( many ) • Trauma and injury. • Neurological syndromes. • Infection e.g. Otitis media or externa, Mastoiditis, Chickenpox ... etc. • Neoplasm. • Toxics. • Metabolic. • Iatrogenic e.g. Mandibular block anesthesia, Antitetanus serum … etc. • idiopathic.
some specific terms in neurology • Dysphonia : is an impairment in the ability to produce voice sounds using the vocal organs. • Diplopia : it means double vision. • Hemianopia : decreased vision or blindness takes place in half the visual field of one or both eyes. • Tone: is the continuous and passive partial contraction of the muscles, or the muscle’s resistance to passive stretch during resting state • Dysarthria : is a speech disorder that is due to a weakness or incoordination of the speech muscles, Speech is slow, weak, imprecise or uncoordinated. • Dysdiadokinesia : an inability to perform rapidly alternating movements, such as regular tapping the fingers on the knee. The cause is a cerebellar lesion.
Paraplegia : is a loss in motor or sensory function of the lower extremities. • Quadriplegia : is paralysis caused by illness or injury to a human that results in the partial or total loss of use of all the limbs. • Hemiplegia : is total paralysis of the arm, leg, and trunk on the same sideof the body i.e. ( paralysis of right half OR left half of the body ). • Diplegia : is paralysis affecting symmetrical parts of the body either arms or legs i.e. ( paralysis of the upper half OR lower half ).
References • Clinical examination 5th edition By Tally. • Illustrated paediatrics by Lissaure and Clayden. • http://www.neuroexam.com/neuroexam/index.php • http://www.youtube.com/user/mootaroo#p/u/5/_1Rd1wVeqU4 • http://reference.medscape.com/
Done by • Dr. WaleedAlotaibi, ( The Hx ). • Dr. EmadA. Kalantan, ( The physical & the neurological conditions ). • Dr. MosheerM. Alzyadi,( Terms in neurology ).