Download
1 / 10
120 likes | 421 Views
Pituitary Adenomas. Elaine Sunderlin, MD PGY-2 Morning Report March 19, 2010. Overview of Pituitary Adenomas. Most common cause of sellar masses from the third decade on Accounts for up to 10% of all intracranial neoplasms Tumors of the anterior pituitary; almost always benign

E N D
Pituitary Adenomas Elaine Sunderlin, MD PGY-2 Morning Report March 19, 2010
Overview of Pituitary Adenomas • Most common cause of sellar masses from the third decade on • Accounts for up to 10% of all intracranial neoplasms • Tumors of the anterior pituitary; almost always benign • Microadenomas: lesions < 1cm • Macroadenomas: lesions > 1cm
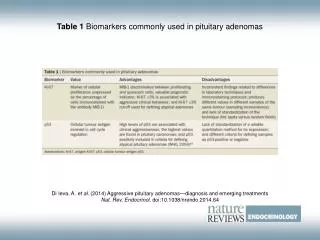
Laboratory Evaluation • Microadenoma • Evaluation for hormonal hypersecretion (prolactin, IGF-1, 24hr urine cortisol/overnight dexamethasone suppression test) • Informal visual field evaluation • Macroadenoma • Evaluation for hormonal hypersecretion (prolactin, IGF-1, 24hr urine cortisol/overnight dexamethasone suppression test) • Evaluation for hormonal hyposecretion (LH, FSH, testosterone) • Formal visual fields
Imaging Evaluation • Nonfunctioning microadenoma (2-4mm) • Likely need no further imaging • Nonfunctioning microadenoma (5-9mm) • MRI can be done once or twice over the subsequent 2 yrs; if stable, frequency can be decreased • Nonfunctioning macroadenoma (< 20mm w/o neurologic abnormalities) • Monitor for adenoma size, visual changes, and hormonal hypersecretion in 6 and 12 months, then annually for a few years
Prolactinoma • Most common hormone-secreting pituitary tumors, approximately 40% of all pituitary tumors • Microprolactinomas more common • Prolactin (PRL) > 200 ng/mL. Levels between 20-200 could be due to a prolactinoma or any other sellar mass • Occur most frequently in females aged 20-50 years, gender ratio of 10:1 • Men: decreased libido, galactorrhea • Women: amenorrhea, galactorrhea • Occasionally prolactin is co-secreted with GH causing clinical syndrome of both prolactinemia and acromegaly
Treatment of Prolactinomas • Regardless of size, medical therapy is first line to obtain normalization of prolactin levels • Dopamine agonists (DA) • Bromocriptine (D2 receptor agonist, D1 antagonist) 2.5-15mg/day divided into 2-3 doses. Occasionally requires doses as high as 20-30mg/day • Normalizes PRL levels, restores gonadal function, and decreases tumor size in 80-90% of microadenomas and 70% of macroadenomas • Cabergoline (D2 selective agonist) 0.5-1mg/week • Works in 95% of microadenomas and 80% of macroadenomas
Surgery • Surgical indications for prolactinomas • Sudden vision disturbance, associated w/ severe HA, altered consciousness and vascular collapse 2/2 apoplexy • Failure of medical therapy (inadequate PRL reduction on high doses of Das or tumor enlargement) • Expanding prolactinomas associated w/ unstable neurological and ophthalmologic deficits unresponding to DAs
Pituitary Apoplexy • Acute infarction or hemorrhage into the pituitary gland • Usually life-threatening emergency • Severe headaches, visual loss, altered consciousness, and impaired pituitary function • Predisposing factors: closed head trauma, blood pressure alterations, h/o pituitary irradiation, cardiac surgery, anticoagulation, treatment with DAs, and pregnancy • The majority of patients present with, at least, partial hypopituitarism. Deficit in ACTH leads to acute glucocorticoid deficiency
Acromegaly Symptoms • Sweaty, oily skin; skin tags; macroglossia • Broadened hands and feets • Jaw thickening, teeth separation, nasal bone hypertrophy • Carpal tunnel syndrome, ulnar nerve neuropathy • Headache • Arthralgias and myalgias
References • UpToDate • Colao, Annamaria. “The Prolactinoma”, Best Practice & Research Clinical Endocrinology & Metabolism;23, 2009;575-596. • Chanson MD, Phillipe, et.al. “Acromegaly”, Best Practice & Research Clinical Endocrinology & Metabolism;23, 2009;555-574 • Murad-Kejbou S, Eggenberg E. “Pituitary apoplexy: evaluation, management, and prognosis”, CurrOpinOphthalmol. 2009,Nov;20(6);456-61 • Chang, Claudia, et.al. “Pituitary tumor apoplexy”. Arq. Neuro-Psiquiatr. vol.67 no.2a São Paulo June 2009