Download
1 / 36
520 likes | 1.23k Views
Chapter 13- leukocyte migration and inflammation. I’ll try VERY hard NOT to be inflammatory!!. Where we’re going-lots of details, so we’ll be hitting the highlights. We’ll frame the subject- LOTS of migration & homing! We’ll learn some CAM’s- cell adhesion molecules

E N D
Chapter 13- leukocyte migration and inflammation I’ll try VERY hard NOT to be inflammatory!!
Where we’re going-lots of details, so we’ll be hitting the highlights • We’ll frame the subject- LOTS of migration & homing! • We’ll learn some CAM’s- cell adhesion molecules • We’ll learn the neutrophil extravasation story, and see a video • We’ll learn some inflammation components, and more of its value • We’ll learn some anti-inflammatory drugs, and their targets.
Leukocytes(PMN's , Mphages, lymphocytes, mainly T) circulate in the blood, but often do their work in tissues. • For T and B cells, circulation increases the chances that you'll meet your antigen. • For both to do their jobs, however, you often have to leave the blood to enter either the lymph node or the site of damage. • Once at the site of damage, you want to kill microbes, control the damage, and repair it.
Lymphocyte recirculation- the circulate a LOT! Your average lymphocyte will make a complete circulation 1-2 times per day Increases the likelihood of meeting Ag.
Key point- mostly activated lymphocytes that are in the tertiary sites. Remember, the gamma-delta lymphocytes are out here
The CAM’s- cell adhesion molecules- key players. Integrins may need to be activated B4 they bind! Think “snot”- and “lectins”- snot-binders! ICAM’s- Ig like VCAM’s- ICAM on endothelial cells
Lots of cytoskeletal rearrangement to slip through the endothelial wall. The endothelium’s inflamed!
Lots of attractants- IL8, C5a, C3a, N-formyl peptides!!!
Lymphocyte extravasation & homing Homing is VERY cool!
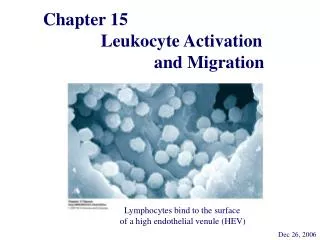
HEV’s- cuboidal rather than flat endothelial cells; 1-2% of venule area, 85% of migration! 14,000/sec!
Key point- skin and intestinal endothelium are not showing the same CAM’s, nor are the effector cells. Homing to tissue, less entry into lymph nodes.
For 3 days after activation, the T cells don’t leave the lymph node (shut-down phase).
Inflammation-where we’re going • Review-The purpose of inflammation is response to injury/infection-usually protective, although not always. • The problem: The components of protection- mphages, neutrophils, antibodies, complement- are mostly in the blood; the damage is often NOT in the blood, but in tissues bathed in interstitial fluid. So inflammation gets the goodies where they are needed. • It also isolates the damage, while bringing effectors to the site (mostly cells), from the blood. • Acute inflammation: five signs- heat, redness, pain, swelling, loss of function.- all related to blood vessel changes.
Mediators of inflammation-injury, clotting, complement all release them • Injury-tissue damage usually accompanies bleeding- bradykinin, the fibrin clot, and its degradation all are inflammatory • These parts interact w/complement (complement can be activated by microbes, of course)- C3a,4a,5a are inflammatory- activate mast cells, histamine, etc.
More… • Tissue damage releases prostaglandins, leukotrienes- membrane components- damage activates enzymes that produce these. Inflammatory, and produce PAIN! • The neutrophils and, particularly, the mphages produce cytokines that stimulate inflammation and a systemic response.
Couldn’t cover this w/o showing you a few prostaglanins… These get whacked off p-lipids from the membrane- the enzymes that do it are activated by signals, damage, etc.
And a few more… From Stryer, Biochemistry
Systemic responses • IL1,IL6, and TNF alpha have systemic effects as well.
Chronic inflammation is BAD! • Continuous Ag stimulation, or so we think • Activated mphages and lymphocytes, producing granulomas and fused mphages- epithelioid cells. Fibroblasts are there, making collagen, interfering with function. • Lymphocytes produce IFN gamma, that stimulates the mphages to produce TNFalpha- kills tumors, but chronic production produces wasting.
Anti-inflammatory drugs • Experimental- Ab's against CAMs- now in clinical trials. Stops extravasation, so slows down inflammation • Corticosteroids- from the adrenal cortex. These cause apoptosis of lymphocytes, reduction of phagocytic ability of mphages/neutrophils • Non-steroidal anti-inflammatory drugs: • Aspirin, Ibuprofen, etc. ONE mechanism is inhibition of prostaglandin synthesis.
This is the simple view- the other one is that it also increases stroke risk. BIG lawsuit about COX-2 inhibitors!
What to know • Lymphocyte circulation- they circulate, but the activated ones are out in the tertiary tissues. • Extravasation story • CAMs- Integrin-ICAM pair, mucin-seLectin pair • Proinflammatory agents from tissue damage, clotting, complement • Proinflammatory cytokines- IL1,6, TNFalpha • Systemic response- fever, acute phase proteins, hematopoiesis • Signs of chronic inflammation • Anti-inflammatory drugs.