Download
1 / 34
350 likes | 780 Views
Genital Urinary System. Female Reproductive System Part 2. Vaginitis. Pathophysiology Vaginitis = inflammation of the vagina Normally pH (3.5-4.5) Maintained by Lactobacillus acidophilus , suppress the growth of anaerobes produces lactic acid i pH Produces hydrogen peroxide.

E N D
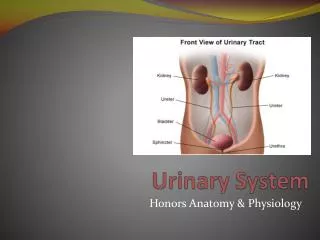
Genital Urinary System Female Reproductive System Part 2
Vaginitis Pathophysiology • Vaginitis = inflammation of the vagina • Normally pH (3.5-4.5) • Maintained by Lactobacillus acidophilus, • suppress the growth of anaerobes • produces lactic acid • ipH • Produces hydrogen peroxide
Vaginitis • Pathophysiology • h risk if… • Stress • Illness • Alt. pH • Pathogen • Candida,Trichomonas or other bacteria invade the vagina.
Vaginitis: Clinical manifestations • Vaginal discharge + • Itching • Odor • Redness • Burning • Edema • Aggravated by voiding • Urethritis (possibly)
Vaginitis: Candidiasis Candidiasis / Vulvovaginal Candidiasis • Fungal or yeast infection • Asymptomatic symptomatic • Use of antibiotics ibacteria i protective organisms • Pg • DM • HIV • Corticosteroid • Oral contraceptives
Vaginitis: Candidiasis Clinical manifestations • Vaginal discharge • Color • White, cottage cheese like • The pH if the discharge is < 4.5 • Pruritus • Itching
Vaginitis: Candidiasis Medical Management • Anti-fungal agents • Miconazole (Monistat) • Without prescription
Bacterial Vaginitis • Overgrowth of anaerobic bacteria normally found in the vagina • Absence of lactobacilli
Characterized by: • Fish-like odor • h vaginal pH • h discharge • Gray –yellowish white • No discomfort
Medical Management • Metronidazole (Flagyl) • PO • Bid x 1wk • Clindamycin (Cleocin) • Vaginal cream
Vaginitis: Trichomoniasis “TRICK” • STD • Sexually transmitted Vaginitis • Asymptomatic carrier
Vaginitis: Trichomoniasis Clinical manifestations • Vaginal discharge • Frothy • Yellow-green • Malodorous • Irritating • Cervical erythema • Multiple small Petechiae • pH > 4.5
Vaginitis: Trichomoniasis • Complications • Not life threatening • Medical Management • Metronidazole (Flagyl) • Anti-bacterial • Anti-protozoal • Both partners!
Nursing process of Patients with Vulvovaginal infection • Assessment • Examine • Do not douche • Observe the area for: • Erytherma • Edema • Excoriation • Discharge
Nursing process of Patients with Vulvovaginal infection • Describe symptoms • Odor • Itching • Burning • Dysuria • Prep vaginal smear • Test pH of discharge
Nursing process Patients w/ Vulvovaginal infection • Assess though questions factors that might contribute to the infections • Physical /chemical factors • Constant moisture from tight or synthetic clothing • Perfumes and powders • Soaps & Bubble baths • Poor hygiene • Feminine hygiene products
Nursing process Patients w/ Vulvovaginal infection • Psychogenic factors • Stress • Fear • Abuse • Medical conditions • DM • Antibiotics • Sex partners
Nursing process Patients w/ Vulvovaginal infection • Diagnosis • Discomfort related to burning, odor or itching from the infectious process • Anxiety related to stressful symptoms • Risk for infection or spread of infection • Deficient knowledge about proper hygiene and preventive measures
Nursing process Patients w/ Vulvovaginal infection • Nursing Interventions • Admin. meds • Sitz baths • Cornstarch powder • Educate patient • Douching discouraged • Loose fitting underwear = good • Tight, synthetic, non-absorbent, heat-retaining underwear = bad
Pelvic Inflammatory Disease Etiology • AKA: Pelvic Infection • PID is an inflammation of the pelvic cavity • Begins with cervicitis uterus, fallopian tubes, ovaries, pelvic peritoneum &/or pelvic vascular system • Usually caused by bacteria • Gonorrheal and Chlamydial organisms • Most common STD but… • Not always STD
PID Pathophysiology • Enters through vagina • Cervical canal • Colonizes • Uterus • Fallopian tubes & ovaries • Pelvis
PID Risk factors • Early age 1st intercourse • h # sexual partners • Sex with a partner with an STD • Hx of STD’s • Previous pelvic infection • Invasive procedure
PID: Clinical manifestation • Vaginal discharge • Dyspareunia • Lower abd. pelvic pain • Tenderness after menses. • Pain h while voiding • Other S&S: • Fever • Gen. malaise • N/V • H/A
PID: Complications • Peritonitis • Abscesses • Strictures / adhesions • chronic pelvic pain
PID: Complications • Fallopian tube obstruction • Ectopic pregnancy • Occlude tubes • sterility
PID:Complications • Bacteremia • septic shock • Thrombophlebitis • embolization
PID: Medical management • Brood spectrum Antibiotics • Treat Partners • Treatment at home • mild • Intensive therapy / Hospital • Rest • IV fluids • IV antibiotics
PID: Nursing Interventions • Activity • Bed rest • Position • Semi-fowler’s • Vital signs • Assess • Drainage • Administer • Analgesics / Antibiotics • Pain relief • Heat to abd.
Endometriosis Etiology • “A benign lesion or lesions with cells similar to those lining the uterus grow aberrantly in the pelvic cavity outside the uterus.” • Chronic pelvic pain & infertility
Endometriosis Pathophysiology • Misplaced endometrial tissue responds to hormone changes • During menstruation, the extopic tissue bleeds, mostly into areas having no outlets pain and adhesions • Causes lesions, cysts and or scar tissue
Endometriosis Clinical manifestations • Dysmenorrhea • Dyspareunia • Pelvic pain • Depression • Loss of work • Relationship difficulty • Infertility
Endometriosis Assessment & diagnostic findings • Health hx • Pelvic exam • Laparoscopy exam
Endometriosis Medical managements • NSAIDS • Oral contraceptives • Side effects: • fluid retention • weight gain • Nausea • Surgery • Pregnancy
Endometriosis: Nursing process • Assessment • Hx & PE focus on specific symptoms, effects of meds, reproductive plans • Diagnosis, Planning and Goals • Relief of pain, Dysmenorrhea, dyspareunia • Avoidance of infertility • Nursing Interventions • Dispel myths and encourage the patient to seek care if dysmenorrhea or dyspareunia occurs • Evaluations/Expected patient outcomes