Download
1 / 29
290 likes | 439 Views
Inequalities in coronary heart disease treatment. Professor Azeem Majeed University College London. Outline of talk. Why CHD is important Inequalities in CHD Inequalities in treatment Possible explanations Proposed solutions. Why is CHD important?. Mortality: Numbers.

E N D
Inequalities in coronary heart disease treatment Professor Azeem Majeed University College London
Outline of talk • Why CHD is important • Inequalities in CHD • Inequalities in treatment • Possible explanations • Proposed solutions
Mortality: Numbers • CHD is the single most common cause of death in both men and women. • One in four men and one in six women die from CHD (about 125,000 deaths in the UK in 2000) • CHD is also the commonest cause of premature death (about 45,000 deaths)
Mortality: International • Death rate from CHD in the UK is among the highest in the world • Although death rates have fallen in the UK, rates have fallen more quickly in many other countries • Within UK, rates are highest in Scotland, Northern Ireland and Northern England
Morbidity: Prevalence • Calendar year 1998 • 210 general practices in England & Wales, part of GPRD • 1.3 million patients
Inequalities: Type • Social Class • Geographical • Ethnic Group
SMR: Social Class • Standardised mortality ratios • Adjust for age (& sex) • Average for population = 100 • Values > 100 imply more deaths than expected • Values < 100 imply less deaths than expected
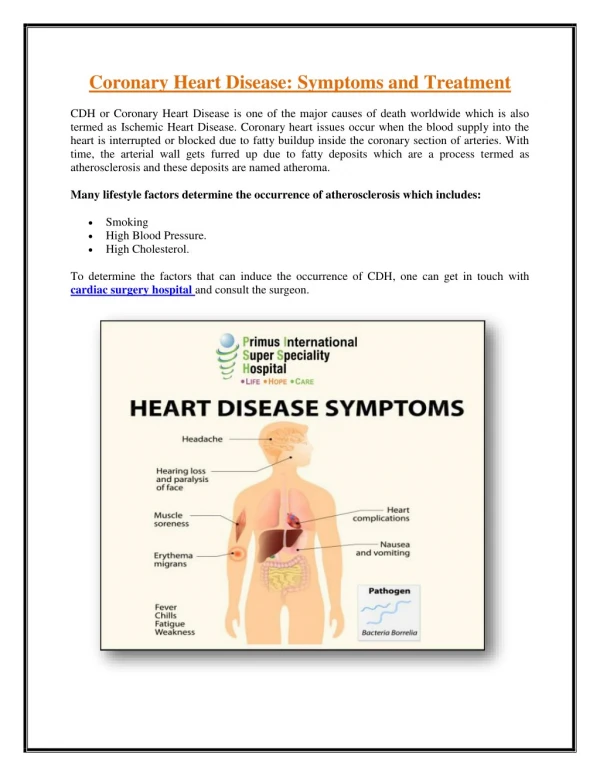
CHD Treatments • Lifestyle changes • Drugs for angina • Drugs to reduce risk of acute events: e.g. aspirin & statins • Control of risk factors: e.g. diabetes, high blood pressure • Interventions: Angioplasty & CABG
Age & sex differences • Calendar year 1998 • 210 general practices in England & Wales, part of GPRD • 1.3 million patients
Study in Wandsworth PCT • 63 general practices • September 2000 - May 2001 • Population 378,000 • 6778 patients with CHD • Some evidence that sex differences narrowing
Secondary & Tertiary Care • Several studies have examined equity of access to care • Thrombolysis • Angiography • Angioplasty & CABG • Drug treatment on discharge
Older studies • Studies carried out in early - mid 1990s • Age, sex and socio-economic differences present • Women, elderly, deprived had poorer access to specialist investigation & treatment
SW Thames: Early 1990s • Admissions for CHD in one year • Proportion of admissions in which angiography carried out • Proportion of admissions in which coronary artery bypass graft (CABG) or percutaneous transluminal angioplasty (PTCA) carried out
Newer studies • Many studies carried out in late 1990s & early 2000s • Show a narrowing of gap between men & women and elderly & younger patients • Possibly still some socio-economic differences in access to specialist care
Possible Explanations • Patient & society • Clinical trials • Primary care • Secondary care • Tertiary care
Proposed solutions • Greater awareness among clinicians and patients • More women and elderly in clinical trials • National service frameworks • Review of health inequalities • Clinical governance • Better use of NHS data for monitoring
Conclusions • Even in a free health care system like the NHS, some groups have poorer access to care than others • Greater awareness among patients, clinicians, policymakers • Interventions in place to reduce inequalities & discrimination