Download
1 / 41
420 likes | 702 Views
Anticonvulsant Therapy. Directed By : Dr. Afaf Al-Arini Presented By : Dr. Y. Abu-zanouna. Anticonvulsant Therapy. Principles of epilepsy treatment Anti Epileptic Drugs Ketogenic diet Surgery for epilepsy. To Treat or Not to Treat ; that is the Question ?.

E N D
Anticonvulsant Therapy Directed By : Dr. Afaf Al-Arini Presented By : Dr. Y. Abu-zanouna
Anticonvulsant Therapy • Principles of epilepsy treatment • Anti Epileptic Drugs • Ketogenic diet • Surgery for epilepsy
To Treat or Not to Treat ; that is the Question ? • Prognosis after the 1st seizure in 1 yr: • 25% risk of having another seizure : neurologically normal, -ve family history,unprovoked siezure. • 37% risk: prior neurological insult (e.g. CP) • After the 2nd seizure : • 70% risk of recurrence .
Anticonvulsant therapy • Withholding treatment until after the second seizure dose not alter the long term prognosis of epilepsy. • Study randomizing 419 patients with 1st tonic-clonic seizure to immediate AED or treatment after a 2nd seizure • Anticonvulsant therapy reduced the short term relapse rate, but at 1 & 2 yrs , the number of seizure- free patients in both groups was similar.
Anticonvulsant therapy • In children with an idiopathic seizure,EEG is the most valuable predictor of recurrence:41% vs. 15 %. • Initial presentation as status epilepticus: The risk of recurrence of any type of seizure is not increased in those with status epilepticus.
To Treat or Not to Treat ; that is the Question ? • Individualized decision. • No treatment: • Another seizure , with the risk of injury , stigma , status epilepticus. • Treatment : • Chronic AED • Cost Of treatment
Anticonvulsant therapy • Practice of most neurologists is to refrain from treatment in 1st idiopathic seizure.In symptomatic seizures treatment is more problematic. • Parents elect to avoid therapy if seizures are infrequent &/or mild. • Absence seizures, drop attacks , infantile spasm are always treated ;they usually present with an established disorder.
Basic principles of AED therapy • Initiation of therapy • Adding a second drug • Monotherapy vs. Polytherapy • Drug-Drug interaction • Anticonvulsant level monitoring
Monitoring serum levels • Onset of treatment • Non-compliant patients & families • At the time of status epilepticus • Patients on polytherapy : D-D • Symptoms & Signs of toxicity • Hepatic or renal disease • Children with cognitive or physical disabilities
Before treatment • Routine blood investigations ? • Family History: • Neurological disease • Consanguinity • Adverse reactions: hematological, cutaneous • Autoimmune disorders • Renal stones
Antiepileptic Drugs: • Drugs that block voltage- dependant sodium channels: • Carbamazepine: • Phenytoin • Lamotrigine • Oxcarbazine
Carbamazepine • Indications: • Used in Generalized tonic-clonic& partial seizures. • Affective disorders : Bipolar disorder • Chronic pain syndromes: trigeminal neuralgia. • Dose: • Begin: 10mg/kg/24h • Increase to 20-30mg/kg/24hr tid
Carbamazepine • Pharmacokinetics; • Absorbed slowly after oral administration • Eliminated by hepatic cyt p450, main metabolite : carbamazepine epoxide • Enzyme inducer • Plasma levels are increased by : erythromycin , clarithromycin , diltiazem , INH
Side Effects • Dose related:Diplopia ,dizziness, ataxia esp in 1st week,GI upset ,tremors, fatigue. • Worsening of myoclonic, atonic & absence seizures,may ppt drop attacks in pt`s with L-G Syndrome. • Allergic : • Skin rash 5-15% • TEN in 1st 8 weeks • Drug induced lupus
Carbamazepine • On chronic use : • Leucopoenia. • Hyponatremia (SIADH) • Heart conduction disturbances. • Advantages • Twice daily extended release forms. • Less teratogenic ( 0.5-1 % )
phenytoin • Used: generalized tonic – clonic , partial seizures , in status epilepticus. • Dose: 3-9 mg/kg/24h bid,oral • Pharmacokinetics:well absorbed,long t1/2 life, peaks in 4-8 hrs • Enzyme inducer • To be adjusted in renal failure
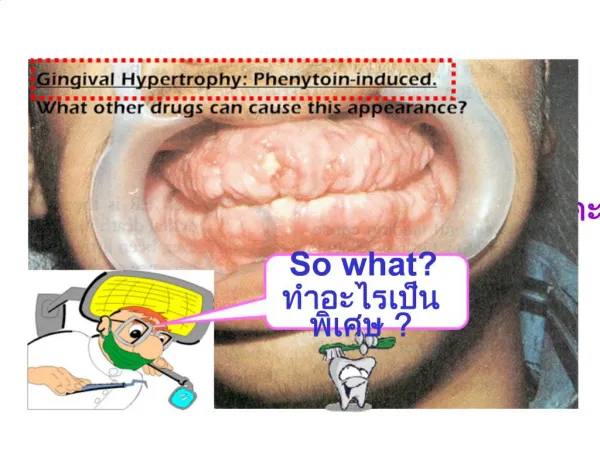
Side effects • Dose related: Nystagmus,drowsiness, fatigue, dysarthria,tremors,impaired concentration,encephalopathy. • Idiosyncratic : skin allergy 5-10% Vasculitis. • Chronic: peripheral neuropathy, behavior changes,coarse facial features, gingival hyperplasia,pulmonary fibrosis,acne,hirsutism,folate deficiency, neonatal coagulation defects,endocrine impairment. • teratogenic
Lamotrigine • Affects neurons that synthesize glutamate & aspartate. • Uses : broad spectrum ,adjunct treatment in generalized seizures & partial seizures,mixed seizures,absence,Lennox-Gestaut • Dose :individualized, based on age & additional anticonvulsants.
Lamotrigine • Side effects: • Dose related: fatigue, ataxia ,drowsiness,nystagmus,insomnia,may cause myoclonic seizures in high doses. • Allergic :TEN,SJS,angioedema(main side effect) • Advantages: • Broad spectrum • Once or twice daily • Not an enzyme inducer • Low teratogenic potential
Oxcarbazepine • Uses : • Polytherapy • Partial seizures • Tonic-clonic seizures • Side effects: • Dizziness ,ataxia,headache ,fatigue • Less hyponatremia than carbamazepine • Teratogenic potential : not known
Antiepileptic Drugs • Drugs that Affect Calcium Currents: • Ethosuximide: • Absence: ( typical better than atypical) • May increase tonic- clonic seizures • Side effects : mainly well tolerated ;GI upset, sleep disturbance , pancytopenia ,lupus-like syndrome.
Antiepileptic Drugs • Drugs that affect GABA metabolism: • Phenobarbital • Clonazepam • Gabapentin • Tiagabine • Vigabatrin
Phenobarbital • Uses : • Generalized tonic – clonic • Partial seizures • Neonatal seizures • Status epilepticus
Phenobarbital • Pharmacokinetics: • T ½ life = 25 – 150 hrs, level is relatively stable , no need for peak & trough levels , no difference. • Serum levels should be checked 3-4 weeks after initial dose ( therapeutic level : 10-40 mcg/ml) • Drug – Drug interaction • Advantages : • Low cost • Once daily • Broad spectrum • IV form
Side Effects • Dose related : Drowsiness, blurred vision , ataxia, fatigue , depression. • Chronic : • Cognitive ,memory & behavioral changes • Megaloblastic changes • Affects vitamin D & calcium metabolism • Withdrawal symptoms on abrupt discontinuation • Coagulation defects in fetus
Clonazepam • Uses : • Absence ,myoclonic, infantile spasm, partial, Lennox- Gastaut , akinetic. • Side effects : • Tolerated in up to 50 % of patients • Drowsiness, ataxia, behavioral & personality changes, excessive salivation.
Gabapentin • Uses : • Add-on-therapy for refractory partial seizures. • Pharmacokinetics: • Excreted unchanged in urine. • Not necessary to monitor serum levels • No drug interactions; 2 hrs after antacids. • Side effects : • Sedation,Dizziness , headache,tremor, nystagmus, weight gain.
Tiagabine • Uses : Infantile spasm,Adjunctive therapy for complex partial seizures. • Side effects: • Idiosyncratic : psychosis or severe depression in 1-2 % • Chronic : Irreversible concentric visual field defect, weight gain • Visual field testing before treatment & every 6 months.
Drugs with multiple mechanisms of action • Valproate : • Mechanism of action: • Blocks voltage – dependant Na channels. • Enhances GABA synthesis • Acts against Ca currents. • Uses : • Broad spectrum AED used alone & in combination for partial seizures & several types of generalized seizures.
VALPROATE • Pharmacokinetics: • Food delays absorption • Drug interactions at protein binding sites • Decreased protein binding in pregnancy ,hepatic & renal disease. • Intravenous preparations now available • Therapeutic levels : 50 –150 mcg/ml ; to be checked after 1-2 weeks.
Side Effects • Fatigue ,tremor,Encephalopathy, alopecia, GI upset. • Idiosyncratic : BM suppression ,pancreatitis,thrombocytopenia. • Hepatotoxicity: higher fatality in children < 2 yrs,& those receiving polytherapy. • Reye like syndrome • Chronic use : weight gain, polycystic ovary. • Teratogenic : NTD in 1st trimester 1-2 %
Topiramate • Mode of action: • Voltage gated Na channels • GABA • Antagonizes glutamate receptors • Week inhibitor of carbonic anhydrase in CNS. • Uses : • Adjuvant therapy for poorly controlled seizures • L-G syndrome
Topiramate • Pharmacokinetics: • Excreted unchanged in urine • Not an enzyme inducer • Therapeutic levels not established • Side effects: • Dizziness , parethesias ,headache. • Chronic use : Wt loss 10 % , nephrolethiasis1-5% . • May increase levels of phenytoin
Stopping antiepileptic treatment • After 2 years with no seizers. • Likelihood of recurrence after 2 years of control 30-40 % • Overall rate of recurrence in idiopathic epilepsy is 29 %. • In symptomatic epilepsy 47 % • Slow EEG on diagnosis 45% • 28% with normal EEG
Life long treatment • Juvenile myoclonic epilepsy • Progressive myoclonic epilepsy • Atypical absence seizures • Lennox-Gastaut
Higher rates of recurrence • Older age at the outset • Syndromes • Symptomatic epilepsy • Poor initial control of seizures • Change in the type of seizures during treatment
Intractable ?? • Consider the following : • Wrong diagnosis. • Inadequate drug level • Inattention to life style factors ( sleep deprivation,alcohol,stress) • Underlying progressive brain disease or metabolic disease. • Intrinsic intractable syndrome. • Wrong drug
Ketogenic Diet • For children with complex myoclonic epilepsy & tonic- clonic convulsions. • Continued for at least two years. • Pyrovate Dehydrogenase deficiency& glucose transport protein deficiency. • Safe for children younger than 2 yrs . • May be unpleasant for older children • ¾ parts fat , 1 part CHO & protein. • Mechanism of action not well known .
Ketogenioc diet • Levels of Ketone bodies to be monitored in serum & urine. • Valproate is contraindicated with this diet. • Suppresses seizure activity by at least 50% in 40% of patients. • Side effects : • Decreased bone mass • Renal stones • Hypoprotenemia • Metabolic Encephalopathy • Hyperuricemia
Epilepsy surgery • Considered, regardless of age , in children with persistent , frequent , refractory seizures , with adverse impact on their lives & interfering with their cognitive , behavioral & psychosocial development. • Focal seizures , with focality documented by EEG,SPECT,PET , fMRI ,MEG.
Epilepsy surgery • Relatively non – invasive : • Vagal nerve stimulation • Invasive : • Local resection • Hemispherectomy • Temporal lobectomy • Corpus callosectomy ( drop attacks )