Download
1 / 15
170 likes | 352 Views
Jaundice. Bilirubin Metabolism. Pre-hepatic Hepatic Post-hepatic. Bilirubin Metabolism: Pre-Hepatic. Bilirubin is formed in reticuloendothelial system as breakdown product of hemaglobin. Heme group biliverdin bilirubin Bilirubin is insoluble in water, bound to albumin.

E N D
Bilirubin Metabolism • Pre-hepatic • Hepatic • Post-hepatic
Bilirubin Metabolism: Pre-Hepatic Bilirubin is formed in reticuloendothelial system as breakdown product of hemaglobin. Heme group biliverdin bilirubin Bilirubin is insoluble in water, bound to albumin. Bilirubin circulates in the blood before uptake by the liver. Pre-hepatic jaundice = if not taken up by the liver/produced in excess, unconjugated bilirubin is deposited in extra-hepatic tissues. Kernicterus in newborns
Bilirubin Metabolism: Hepatic • Bilirubin is taken up into hepatocytes and conjugated to glucuronic acid = bilirubin diglucuronide > bilirubin monoglucuronide > secreted into bile • The glucuronide conjugated form of bilirubin is water soluble and is excreted into bile. • Hepatic jaundice = disorders of bilirubin uptake or conjugation
Bilirubin Metabolism: Post-Hepatic • Glucuronide-conjugated bilirubin degraded to urobilinogen. • Urobilinogen pathway: • may be reabsorbed by the gut and returned to the liver • converted to urobilin > reabsorbed into plasma for excretion by kidneys • May be acted upon by bacterial enzymes within the gut to form the bile pigment stercobilinogen > stercobilin>brown color of feces • Obstructive jaundice = failure of bilirubin to reach the gut > light colored stool, dark urine.
DDX: Conjugated Hyperbilirubinemia Intrahepatic Cholestasis (impaired excretion) Functional, obstructive Hepatitis (viral, alcoholic, and non-alcoholic) Primary biliary cirrhosis or end-stage liver dz Sepsis and hypoperfusion states TPN Pregnancy Infiltrative disease: TB, amyloid, sarcoid, lymphoma Drugs/toxins i.e. chlorpromazine, arsenic Post-op patient or post-organ transplantation Hepatic crisis in sickle cell disease
DDX: Obstructive Jaundice Extrahepatic Cholestasis (obstructive jaundice) Choledocholithiasis Cancer/Neoplasm: Pancreatic CA Cholangiocarcinoma (rare) Gallbladder CA Ampullary adenoma/adenocarcinoma Duodenal adenoma/adenocarcinoma Metastatic CA (and adenopathy of porta hepatis) Strictures after invasive procedures Acute and chronic pancreatitis Primary sclerosing cholangitis (PSC) Parasitic infections
Evaluation: History Fever/chills, RUQ pain (cholangitis) Use of alcohol Hepatitis risk factors Inherited disorders including liver diseases and hemolytic conditions H/O blood transfusion TPN use H/O abdominal surgery Travel history Use of drugs or herbal medications Exposure to toxic substances
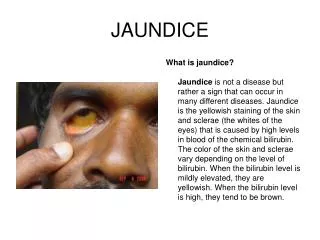
Evaluation: PE Look for jaundice: under tongue, conjunctiva, skin (>1.5mg/dL) Signs of end stage liver disease (cirrhosis): ascites, splenomegaly, spider angiomata, and gynecomastia Hyperpigmentation (hemochromatosis) Kayser-Fleischer ring (Wilson’s disease) Courvoisier’s sign = painless, palpable/distended gallbladder on exam (think of CA)
Evaluation: Labs CBC – infection, anemia LFTs Bilirubin (total/direct/indirect) AST, ALT (AST/ALT) Predominant increase in AST/ALT implies intrinsic hepatocellular disease Alk Phos, GGT ↑Alk Phos also seen in sarcoid, TB, bone In this case, GGT is specific for biliary origin INR/albumin CA 19.9 AFP
Evaluation: Additional Labs Further specific labs. Serologic tests for viral hepatitis Antimitochondrial antibodies (for primary biliary cirrhosis) Anti-nuclear anti-smooth muscle (sm), and liver-kidney microsomal (LKM) antibodies (for autoimmune hepatitis) Serum levels of iron, transferrin, and ferritin (for hemochromatosis) Serum levels of ceruloplasmin (for Wilson's disease) Measurement of alpha-1 antitrypsin activity (for alpha-1 antitrypsin deficiency)
Imaging for Obstructive Jaundice RUQ U/S: Stones, wall thickening, edema, CBD diameter/obstruction MRCP ERCP Direct visualization of biliary tree & pancreatic ducts Procedure of choice for choledocholithiasis Diagnostic & therapeutic PTC When ERCP not possible CT scan: identification and description of obstruction Endoscopic U/S: visualization of the common bile duct without the hindrance of overlying bowel gas
Treatment Start with ABCs & resuscitation If obstructive jaundice: Ascending cholangitis: IVF, ABX, decompression (medical emergency) Stones: remove using ERCP or surgery Benign stricture: stent vs. drainage catheter Cancer: Stent vs. drainage +/- resection of CA Primary goal = decompression
Take Home Points Jaundice DDX is extensive DDX starting point: pre-hepatic, hepatic, post-hepatic Obstructive jaundice: choledocholithiasis, tumors, PSC, pancreatitis, stricture, parasites Ascending cholangitis is an emergency that must be identified and treated promptly Imaging: U/S, EUS, CT, ERCP, MRCP Treatment of obstructive jaundice: decompression