Download
1 / 12
140 likes | 350 Views
Benign Prostatic Hyperplasia. Dr.Bandar Al Hubaishy Urology Department KAUH. Clinical Presentation. Hesitancy Urgency Frequency Incomplete bladder emptying Drippling Decreased stream flow. Physical Examination. Suprapubic area for sign of bladder distension DRE: Prostate gland

E N D
Benign Prostatic Hyperplasia Dr.Bandar Al Hubaishy Urology Department KAUH
Clinical Presentation • Hesitancy • Urgency • Frequency • Incomplete bladder emptying • Drippling • Decreased stream flow
Physical Examination • Suprapubic area for sign of bladder distension • DRE: Prostate gland size , nodularity , masses, surface, tenderness, anal tone
Laboratory tests: CBC U&E PSA Urine analysis Urine culture and sensitivity Uroflow meter Kidney-bladder Ultrasound TRUS biopsy investigations
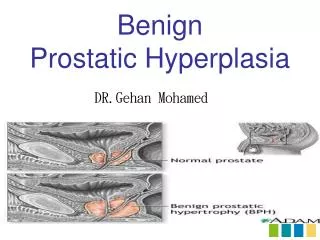
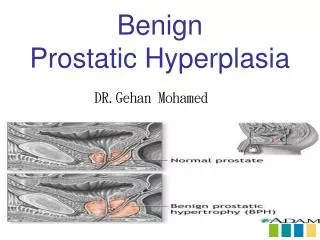
Medical Treatment • The prostate gland consists of : • Glandular tissue • Fibromuscular tissue
Medical Treatment • The prostate is rich in alpha receptors especially type 1a which are responsible for LUTS in those patient. So, blocking these receptors can decrease the resistance along the bladder neck, urethra and prostate
Selective agents short-acting: prazosin, alfuzosin, and indoramin. long-acting: terazosin, doxazosin and slow-release (SR) alfuzosin. Non selective agents Phenoxybenzamine Partial selective agents Tamsulosin and silodosin. Alpha blockers
5 alpha reductase inhibitors • Finasteride (Proscar) • Dutasteride (Avodart)
Indications: AUR failed voiding trials recurrent gross hematuria urinary tract infection. renal insufficiency secondary to obstruction. failure of medical therapy, a desire to terminate medical therapy financial constraints associated with medical therapy. Surgical management
Transurethral resection of prostate (TURP) Complications: Hemorrhage, urinary incontinence, impotance, retrograde ejaculation
Open prostatectomy Indications : • very large prostates (>75 g), • patients with concomitant bladder stones or bladder diverticula • patients who cannot be positioned for transurethral surgery.