Download
1 / 26
280 likes | 861 Views
Benign Prostatic Hyperplasia. Anoop Agrawal, M.D. Baylor College of Medicine Med-Peds Continuity Clinic. Prevalence of BPH. AUA BPH Algorithm. Medical History. Seven cardinal symptoms: urinary frequency nocturia urgency hesitancy weak straining to void sensation of incomplete voiding.

E N D
Benign Prostatic Hyperplasia • Anoop Agrawal, M.D. • Baylor College of Medicine • Med-Peds Continuity Clinic
Medical History • Seven cardinal symptoms: • urinary frequency • nocturia • urgency • hesitancy • weak • straining to void • sensation of incomplete voiding
Initial Evaluation • History • Digital Rectal Exam & Focused Physical • Urinalysis • PSA • AUA Symptom Index Score
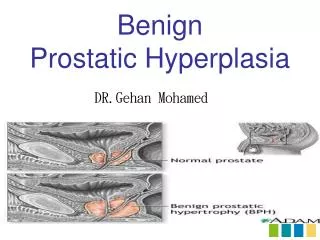
BPH: Diagnosis • Palpable prostate size does not correlate with a diagnosis of BPH, nor with degree of obstruction or the severity of symptoms. • Use urinary symptom scoring scale by the American Urological Association to aid with diagnosis. • consists of seven questions - each question grades severity of each symptom
Differential Diagnosis • Diabetes • UTI • Neurogenic bladder • Urethral strictures • Cancer (bladder or prostate) • Medication induced
Laboratory Testing • Urinalysis • PSA • Optional tests: • urinary flow rate measurements • postvoid residual urine measurements • pressure flow studies
AUA Symptom Index: Interpretation • Classification: • Mild: 0-7 • Moderate: 8-19 • Severe: 20-35 • The AUA score needs to be put in the context of whether the condition is or is not bothersome.
Treatment • Studies have found that over a follow-up period of 2.6 to 5 years, 16% men had stable symptoms and 38% improved over time. • Treatment choices must take into account: • Symptom Index Score • Effect on quality of life
Case One • A 62 yo man reports nocturia, frequency and urgency. His UA is negative, PSA is normal. His AUA Severity Index is 10. He states the symptoms are not very bothersome. What treatment options do you recommend? • A. Watchful waiting • B. alpha-1 blocker • C. 5-alpha reductase inhibitor • D. Surgical therapy
Case One • A 62 yo man reports nocturia, frequency and urgency. His UA is negative, PSA is normal. His AUA Severity Index is 10. He states the symptoms are not very bothersome. What treatment options do you recommend? • A. Watchful waiting • B. alpha-1 blocker • C. 5-alpha reductase inhibitor • D. Surgical therapy
Treatment • Though symptom score may be above the Mild range (0-7), initiating medical therapy is not warranted unless patient finds he is bothered by the symptoms. • May begin with behavior modifications: • reducing fluid intake at night • reducing consumption of mild diuretics (caffeine and alcohol)
Treatment • Alpha-1 Blockers - common first line agent • Rapid onset, reduction in symptom score by 30-40% • Nonselective Alpha-1 Blockers • SE: dizziness, orthostatic hypotension, fatigue, asthenia; occurs in 7-9% • Selective Alpha Blocker (tamsulosin, alfuzosin) - less anti-hypertensive effect
Case Two • A 59 yo male presents with symptoms of BPH. His rectal exam reveals a enlarged prostate. You estimate at least 40 grams in size. His AUA score is 16. He reports the symptoms are very bothersome. What treatment options do you recommend? • A. Watchful waiting • B. alpha-1 blocker • C. 5-alpha reductase inhibitor • D. Surgical therapy
Case Two • A 59 yo male presents with symptoms of BPH. His rectal exam reveals a enlarged prostate. You estimate at least 40 grams in size. His AUA score is 18. He reports the symptoms are very bothersome. What treatment options do you recommend? • A. Watchful waiting • B. alpha-1 blocker • C. 5-alpha reductase inhibitor • D. Surgical therapy
Treatment: Case Two • 5-alpha reductase inhibitors (finasteride, dutasteride) these require long-term treatment (6-12 months) before symptom improvement is seen • more effective in men with large prostate • Combination therapy with alpha-1 blocker and 5-alpha reductase inhibitors • found to be effective in men with severe symptoms or men with moderate symptoms and large prostate • Downside is that long-term safety of finasteride is unknown
Combination Therapy in BPH McConnell, JD, Roehrborn, CG, Bautista, OM, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med 2003; 349:2387
Case Three • A 65 yo man with moderate symptoms of BPH is worried about side effects from alpha-1 blockers and wants to know if any herbal remedies are recommended. What do you advise?
Case Three • Complementary Medicine options • Genistein - an isoflavone found in tofu/soy products, found to decrease growth of hyperplastic prostate tissue in histoculture, marketed as Trinovin, dose 40 to 80mg qd. • Saw palmetto - few side effects, safe, dosage is 160mg bid • A 2006 prospective trial found no improvement in symptoms. Current recommendation is to avoid.
Case Four • A 55 yo man has been experiencing chronic intermittent hematuria for past several months. Urology performed a flexible cystoscopy revealing no evidence of malignancy or atypia. PSA is normal. What treatment option is available to suppress gross hematuria? • Finasteride - randomized trial of 57 men had lower rate of recurrent hematuria (14 vs 63%)
Surgical Treatments • Open prostatectomy • Transurethral Resection of the Prostate (TURP) • Transurethral Incision of the Prostate (TUIP) • Transurethral Microwave Thermotherapy (TUMT) • Transurethral vaporization of the prostate (TUVP) • Transurethral needle ablation of the prostate (TUNA)
Conclusion • Diagnosis based upon patient’s symptom index and affect on quality of life • Wide range of treatment options - discuss with patient benefits and risks. • Surgical therapy tends to be more effictive, but results in more residual side effects.
References • Bent S, et al. Saw Palmetto for Benign Prostatic Hyperplasia. NEJM 2006; 354:557-566. • Dull P, et al. Managing Benign Prostatic Hyperplasia. Am Fam Physician 2002;66:77-84. • UpToDate 2009: Medical Treatment of benign prostatic hyperplasia. (Accessed February 21 & 22, 2009).