Download
1 / 23
300 likes | 1.27k Views
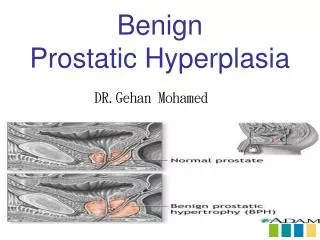
Benign Prostatic Hyperplasia. Objectives. Upon Completion of this CME activity, the learner will be able to: Understanding the current medical management for BPH. BPH. Definition: Proliferation of the fibrostromal and glandular tissue of the prostate Not mutually exclusive to LUTS or BOO

E N D
Objectives • Upon Completion of this CME activity, the learner will be able to: • Understanding the current medical management for BPH
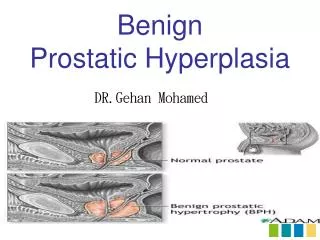
BPH • Definition: Proliferation of the fibrostromal and glandular tissue of the prostate • Not mutually exclusive to LUTS or BOO • Typically found in men over age 60 (50%) • Age 85 (90%)
BPH • Clinical Features: • Obstructive Sx = weak stream, hesitancy, straining, post void dribbling, sensation of incomplete emptying • Irritative Sx = frequency, nocturia (most common), urgency
Progression • BPH does not progress in all patients • In men with mild LUTS, 57% progress to worse LUTS in 4 yrs • 30% remain stable • 15% improve • Only 10% progress to needing surgical intervention • The risk of BPH progression is higher in men with… • Larger prostate size • Higher PSA • Older age • More severe LUTS
BPH Complications • Detrussor dysfunction • Urinary retention • Hematuria • UTI • Renal failure • Bladder calculi
Evaluation • Non-Invasive Evaluation • Medical History • AUASS • DRE • UA • PSA • Voiding Diary • PVR • Uroflow • Creatinine
Evaluation • Invasive Evaluation • Pressure Flow study • Cystoscopy • TRUS
Diagnosis • Severity of BPH symptoms do not correlate with prostate size or the degree of bladder outlet obstruction • Men with small prostates can have severe symptoms, etc • Keys to diagnosis are… • Determining if there is Bladder Outlet Obstruction • Low flow on uroflow • Elevated post-void residuals • Trabeculation of bladder on cystoscopy • Low flow rate and high detrusor pressure on urodynamics • DRE and PSA level are not absolute • Must rule out infection and cancer which can cause similar symptoms
Management • Conservative Measures • Avoid substances that can exacerbate symptoms • α-agonists – decongestants that contain pseudoephedrine • Anticholinergics in some cases • Caffeine / alcohol / spicy or acidic foods • Reducing nocturia • Decreasing nightly fluid intake • Avoiding diuretics in evening • Elevating legs before bedtime for those with LE edema
Management • Medications • α-Blockers • 5α-Reductase Inhibitors • Combination Therapy • Mostly commonly will progress to surgery if… • Patients are tired of taking medications • Symptoms present despite medications
Medications • α-Blockers • Terazosin (Hytrin) • Doxazosin (Cardura) • Flomax • Rapaflow (most RGE) • Uroxatral (least RGE) α-1 selective Nonselective α-blockers Dose dependent response α-1A and D selective
Medications • α-Blockers • Hytrin, Cardura, Flomax, Uroxatral, Rapaflow • They relax the smooth muscle of the prostate stroma • Maximal response is usually 1-2 weeks • Side effects include: • Dizziness, fatigue, nasal congestion, syncope, orthostatic hypotension, retrograde ejaculation, intraoperative floppy iris syndrome w/ cataract surgery • Hytrin / Cardura may also be used to treat HTN • Must also counsel pts on possibility of hypotension when combining PDE-5 inhibitors with nitrates or α-blockers.
Intraoperative Floppy Iris Syndrome (IFIS) • Recommendation: Men with LUTS secondary to BPH for whom alpha blocker therapy is offered should be asked about planned cataract surgery • Men planning surgery should avoid them until cataract surgery is completed • In men with no planned cataract surgery, there are insufficient data to recommend withholding or discontinuing alpha blockers
Medications • 5α-Reductase Inhibitors • Finasteride (Proscar) Type II Inhibitor • Dutasteride (Avodart) Type I & II Inhibitor • They prevent conversion of testosterone to DHT • Reduce serum DHT levels by 70-90% and prostatic DHT levels by 80-95% • THEY TAKE SIX MONTHS TO WORK!!
Medications • 5α-Reductase Inhibitors • Proscar, Avodart • They lower DHT and promote… • Reduces prostate volume by 20-25% • Increases maximum flow rate by 10% • Improves urinary symptom score by 20-30% • Reduces risk of urinary retention by 50% • Reduces need for surgical therapy by 50% • Reduces the risk of BPH progression by 34% • Reduces PSA by 50% after 6 months (no decrease think cancer) • If on these meds, need to double PSA when looking at CaP screening • May help stop chronic hematuria from prostate • Can be used for bleeding prevention in TURP
Medications • Combination Therapy • Medical Therapy of Prostate Symptoms (MTOPS) Trial (McConnell, et al, N Engl J Med, 2003) • 3047 men Age > 50 yrs Mean F/U 4.5 yrs • Cardura vs. Proscar vs. Both • Greatest benefit in men w/ PSA > 4.0 & Prostate Volume > 40 cc
Medications • CombAT trial • Compared tamsulosin, dutasteride and combination • Combination showed better flow, AUASS and reduced progression compared to tamsulosin alone
Medications • Complimentary Therapies • AUA does not recommend these as standard therapy • Mechanism of action is unknown or if they change PSA • Sal palmetto is most widely used • Others include: African plum tree, Pumpkin seed, African star grass, Rye pollen, Stinging nettle
Management • Surgical Options: • Minimally Invasive Surgical Therapy (MIST) • TUNA, TUMT, or HIFU • Not currently offered at NMCP • TUIP, TURP, and Open Simple Prostatectomy • TURP vs. Vaporization • Traditional resection with a cutting loop • Photovaporization of the Prostate • Plasma button vaporization of the prostate • Holmium laser enucleation of the prostate