Download
1 / 58
690 likes | 1.58k Views
BENIGN PROSTATIC HYPERPLASIA. DR .MOHAMMAD H DUMIRIEH. 2014. DEFINTION. Hyperplasia of stroma and epithelium in periurthral area of prostate (transition zone) Tone of prostatic smooth muscle plays role in addition to hyperplasia. ETIOLOGY. Etiology unknown

E N D
BENIGN PROSTATIC HYPERPLASIA DR .MOHAMMAD H DUMIRIEH 2014
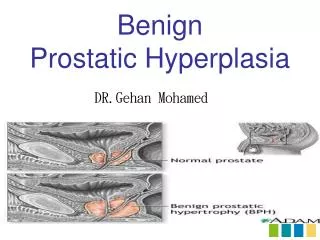
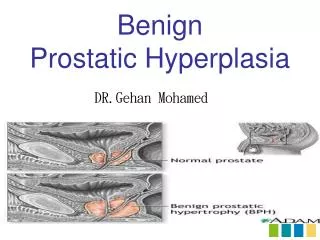
DEFINTION • Hyperplasia of stroma and epithelium in periurthral area of prostate (transition zone) • Tone of prostatic smooth muscle plays role in addition to hyperplasia
ETIOLOGY • Etiology unknown • Androgen dihydrotestosterone(DHT)required (converted from testosteron by 5-alpha reductase) • Possiple role of impaired apoptosis, estrogen. other growth factors
Epidemiology • Age related,extremly common(50% of 50 year olds,80% of 80 year olds) • 25 % of men will require treatment
Clinical Feature • Reslut from outlet obstruction and compensatory changes in detrusor function • Voiding symptoms: .hesitancy,straining,weak/interrupted stream,incomplete bladder emptying .decreased flow rates may be seen on uroflowmetry. .due to out flow obstruction and/or impaired detrusor contractility.
Clinical Feature • storage symptoms: .urgency,frequency,nocturia,urgency incontinence .thought to be due to detrusoroveractivity and decreased compiliance.
Prostate is smooth ,rubbery and symmeetrically enlarged on DRE • Complication: - Retention - Overflow incontinence - Hydronephrosis and renal compromise
Complication: - infection - gross hematuria - bladder stones
AUA prostate symptom score • funwise
funwise • frequency • urgency • nocturia • Weak stream • intermittency • straining • Emptying,incomplete feeling
Each symptom graded out of 5 0-7 mildy symptomatic 8-19-moderately symptomatic 20-35 severely symptomatic Note: dysuria not included in score but is commonly associated with BPH
APPROXIMATE PROSTATE SIZE 20cc-chestnut 25cc –plum 50cc-lemon 75cc-orange 100cc-grapefruit
investigation • history • Assess LUTS and effect on quality of life ,may include self –administredequestionnires (AUA symptom and impact score) • Physical exam:DRE • Urinalysis to exclude UTI • Creatinine to assess renal function +-renal ultra sound to assess for hydronephrosis. • PSA to rule out malignancy (if life expectancy more than 10 y)
investigation • Uroflowmetry (optional) • Bladder ultra sound post voiding urine(optional) • Cystoscopy prior to potential surgical management. • Biopsy if suspicious for malignancy
TREATMENT • Conservative for those with mild symptom: .watchful waiting-50% of patients improve spontaneously. .includes lifestyle changes(e.g evening fluid restriction,planned voiding)
Medical treatment: .a-adrenergic antagonist-reduce stromal smooth muscle tone .5-a reductase inhibitor _block conversion of testosteron to DHT;acts on the epithelial component of prostate –reduces prostate size[e.g.finastride(proscar),dustride(avodart)]
Objective • To partially resect the periurethral area of prostate (transition zone)to decrease symptoms of urinary tract obstruction.
Indications • Obstructive uropathy (large bladder diverticula ,renal insufficiency) • Refractory urinary retention • Recurrent utis • Recurrent gross hematuria • Bladder stone • Failure of medical therapy
complication • Acute: *intra or extraperitoneal rupture of bladder *rectal perforation *incontinence *hemorrhage *epididymitis *sepsis
*trance urethral resection syndrome(post –TURP) .caused by absorption of large volume of hypotonic irrigation solution used ,usually through perforated venous sinusoid,leading to hypervolemichyponatremicstate.
.characterized by: dilutionalhyponatremia ,confusion,nausea,vomiting,hypertension,visualdistrubance,pulmonaryedema,bradycardia. .treat with diuresis and (if severe)hypertonic saline administration
complication • chronic: *retrograde ejaculation(>75%) *erectile dysfunction(5-10% risk increase with increasing use of cautery) *incontinence(<1%) *urethral stricture *bladder neck contracture.
Open prostatectomy: .for large prostates or assochiated problems(e.g.bladder stones) .suprapubic (transvesically to deal with bladder pathology) .retropubic(through the prostatic capsule)
Absolute indication for surgery • Refractory urinary retention • Recurrent utis • Recurrent hematuria refractory to medical treatment • Renal insufficiency (rule out other causes) • Bladder stones
Simple prostatectomy ALMOUSATE HOSPITAL
Minimally invasive therapy .prostatic stent, microwave therapy , laser ablation, water –induced thermotherapy, cryotherapy, high intensity focoused ultra sound (HIFU), transurethral needle ablation (TUNA).
Stent within prostate • The passage way is wide and the lumen of bladder clearly seen
PSA • Enzyme produced by epithelial cells of prostate gland to liquify the ejaculate • Leaks into circulation and is present < 4ng/ml • Measuerd total serum PSA is a combination of free(unbound)PSA (15%)and complexed PSA(85%)
Screening Prostate cancer : PSA and DRE • PSA may be elevated in prostate cancer and many other condition; not specific to cancer • Population –based ,routine screening not recommended
Must discuss risk factors,test characteristic , risk of over-detection and over treatment,treatment and active surveillance • Well –informed patients can elect to undergo PSA and DRE
The decision to proceed to prostate biopsy should be based primarily on PSA and DRE results,but should take into account multiple factors (free and total PSA,patientage,PSAvelocity,PSAdensity,familyhistory,ethnicity,prior biopsy history and comorbidities)
PSA is specific to the PROSTATE, but not to prostate cancer.
In PSA testing , think “free and easy” : increased free/total ratio suggests benign cause of high PSA
Causes of Increased PSA • BPH,prostatitis,prosatic ischemia /infarction • Acute urinary retention, prostate biobsy/surgery/ message • Urethral catheteraization,TRUS • Ejaculation ,acute renal failure • Coronary bypass graft. • Radiation therapy
*free-to –total PSA ratio: • Complexed PSA increases in prostate cancer,decreasing the percentage of the free fraction • <10% free PSA suggestive of cancer ,>20% free suggest benign cause
*PSA velocity: • Change of >0.75ng/ml/year associated with increased risk of cancer
*PSA density: • PSA divided by prostate volume of as found on TRUS • >0.15 ng/ml/ associated with increased risk of cancer