Download
1 / 36
360 likes | 616 Views
Human Immunodeficiency Virus. By: Dr.Mona Badr. Assistant Professor & Consultant Virologist College of Medicine & KKUH. Human Immunodeficiency Virus. Retroviridae family is divided into three subfamilies:

E N D
Human Immunodeficiency Virus By: Dr.Mona Badr Assistant Professor & Consultant Virologist College of Medicine & KKUH
Human Immunodeficiency Virus • Retroviridae family is divided into three subfamilies: • Oncovirinae includes human T-lymphotropic virus types 1 & 2 (HTLV-1 Adult T-cell leukemia • (HTLV-2 No human infection) • Lentivirinae includes HIV 1 Worldwide AIDS (Pandemic) HIV2 West Africa AIDS • Spumavirinae No human infection
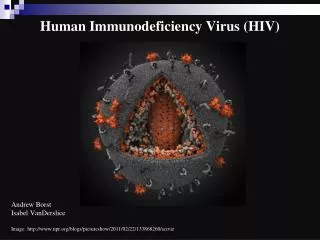
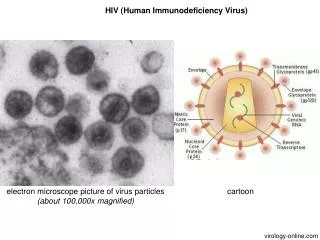
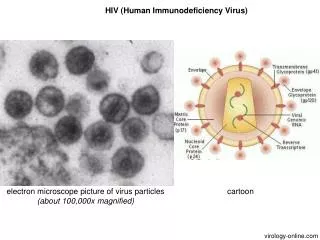
Human Immunodeficiency Virus (Continued) • HIV consists of an outer envelope covered with glycoprotein spikes. • An internal core genome consists of two identical ss-RNA genome of which enzyme reverse transcriptase is bound. • The viral genome has 3-structural genes termed • gag core , • Env (envelop) • Pol (Reverse Transcriptase)
Human Immunodeficiency Virus (Continued) • HIV is known to infect mainly T-helper cells and macrophages. • Destroying T-helper cells results and severe immunologic impairment, leading to multiple opportunistic infections, unusual cancers and death.
Human Immunodeficiency Virus Transmission: • Sexually: • By sexual contact especially homosexual • The virus is present in semen and vaginal secretions • Parenterally: • Direct exposure to infected blood and blood products. • Use contaminated needles and syringes as in (drug abuser) and Tattooing. • Through contaminated surgical and dental instruments. • Sharing contaminated razors and tooth brushes, nail cutters.
Human Immunodeficiency Virus (Continued) Transmission: • From mother to child • Infected mother transmit HIV to their babies in approximately 15-30% of cases. Treatment of the mother with antiviral therapy can prevent this in mostcases. • HIV is transmitted from mother to child ,in utero, during delivery or perinatally via breast feeding.
Virus Inactivation • HIV is easily inactivated by treatment for 10 min at 37oC with any of the following • 10% house hold bleach, Sodium Hypochlorite • 50% ethanol • 35% isopropanol • 0.5% Paraformaldehyde • 0.3% hydrogen peroxide
The Course of HIV-infection • The course of HIV-infection can be divided into three stages: • The acute phase • The chronic phase • AIDS
The Course of HIV-infection • The acute phase • Incubation period 1-4 weeks • Mostly asymptomatic, in 25-50% of cases patients may have symptoms resembling infectious mononucleosis or influenza like illness for short period. • Characterized by the appearance of HIV-Ag in the blood (p24 Ag core Ag) followed by: • Appearance of two antibodies, one directed to the envelope and the other to the core proteins
The Course of HIV-infection (Continued) • The chronic phase • This phase totally asymptomatic, which lasts for about 1-10 years in adults, 1-5 years in children. • Characterized by the disappearance of HIV-Ag (p24) from circulation and the presence of anti-envelope and anti-core. • CD4 counts are generally within normal limits (usually above 350 x106 cells/L) • At the end of this stage, two syndromes appear: • Persistent generalized lymphadenopathy (PGL) • AIDS-related complex (ARC)
The Course of HIV-infection(Continued) • Persistent Generalized Lymphadenopathy: • Is present in 25-30% of patient who are otherwise asymptomatic. • Enlarged lymph nodes (at least 1 cm in diameter), in two or more non-contagious extra-inguinal sites, persisting for at least 3-months in the absence of any other illness or medication known to cause enlarge lymph node Blood markers: • HIV Ag p24 (indicate active viral replication) • Anti-envelop +ve • Anti-core –ve • CD4 count but still >200 x106 cells/L
The Course of HIV-infection (Continued) • AIDS-related complex (ARC): • Are indicative of a defect in cell-mediated immunity and often manifested as candidiasis(oral thrush) seborrhoeic dermatitis,and disseminated zoster (shingles). • .constitutional symptoms; • Fever, diarrhea persisting more than a month with weight loss greater than 10% (Slim disease), night sweat, fatigue and malaise • Neurological disease as myelopathies and peripheral neuropathy.
The Course of HIV-infection (Continued) Blood markers: • HIV Ag +ve( p24 indicate active viral replication) • Anti-envelop +ve • Anti-core -ve • Decrease count of CD4but still more than 200 x106 cells/L
The Course of HIV-infection (Continued) Blood markers: • HIV Ag +ve( p24 indicate active viral replication) • Anti-envelop +ve • Anti-core -ve • Decrease count of CD4but still more than 200 x106 cells/L
The Course of HIV-infection (Continued) • AIDS • The end stage of the disease characterized by: • Marked decrease in CD4 T-helper cells < 200 x 106 cells/L • Severe immunologic impairment, cell mediated immunity • Opportunistic infections e.g. pneumocystis carinii pneumonia, toxoplasmosis of brain, disseminated or extra pulmonary mycobaceriosis etc. • Unusual cancers (Kaposi’s sarcoma)
Blood markers • HIV Ag +ve( p24 indicate active viral replication). • . • . • Anti-envelop +ve • Anti-envelop +ve
Laboratory Diagnosis Confirming W.B. Riba HIV Ag p24 PCR Screening Elisa HIV-antibody
Laboratory Diagnosis • By detection of both HIV-Ab and HIV-Ag, using EISA (screening test) • If results are negative, report negative • If results are positive, repeat the screening test in duplicate(twice) • Repeatedly reactive specimens, must be confirmed by Western blot and HIV-Ag test by Eliza. • If the confirmatory results are negative, report negative • If the confirmatory test results are positive, report positive
Laboratory Diagnosis (Continued) Western Blot: • To confirm the presence of Anti –HIV to the structural proteins of the virus gag core protein env. envelop Protein pol reverse transctpise HIV Ag p24: • To confirm the presence of the major protein of the core. PCR: • For detection of HIV RNA in the blood by using reverse transcriptase.
Treatment • Treatment does not eradicate the virus, but suppress the HIV replication. • Treatment, should continue all life • The aim of treatment is to maintain the immune system of the treated patient near normal as possible • At the present time the combined therapy is used two reverse transcriptase inhibitors pulse one protease inhibitor
Treatment (Continued) • Reverse Transcriptase Inhibitors: • AZT Zidovudine • ddC Zalcitabine • ddI Didanosine • d4T Stavudine • 3TC Lamivudine • All the above anti-viral drugs are nucleoside analogues. • Protease inhibitors • Saquinavir • Indiniavir • Ritonavir • Nelfinavir
Treatment (Continued) Prevention & Control: • There is no vaccine available yet for HIV • Practice safer sex by having one sexual partner • Do not share razors, tooth brushes, etc • Do not share needles and syringes • Avoid direct exposure to body fluids • Educate the public about HIV-infection • Significant reduction in mother-to –child HIV transmition if ZIDOVUDINE is given during pregnancy OR NEVIRAPINE given as a single dose during delivary.