Download
1 / 30
410 likes | 1.57k Views
Respiratory Physiology . Chapter 16. Objectives of Chapter 16. To understand the: Structure and function of the lungs Mechanics of breathing Assessment of pulmonary function Principles of gas exchange. Respiration. Encompasses 3 related functions: Ventilation : breathing

E N D
Respiratory Physiology Chapter 16
Objectives of Chapter 16 To understand the: • Structure and function of the lungs • Mechanics of breathing • Assessment of pulmonary function • Principles of gas exchange
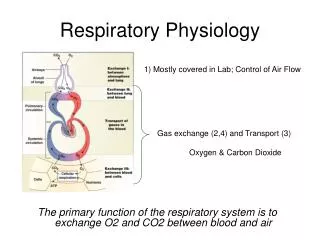
Respiration • Encompasses 3 related functions: • Ventilation: breathing • Gas exchange: occurs between air and blood in the lungs and between the blood and body tissues • Oxygen utilization: cellular respiration Ventilation: • Externalrespiration – ventilation moves air in and out of lungs for gas exchange with blood • Internal respiration – gas exchange between the blood and other tissues, and O2 use by tissues • Gas exchange is passive via diffusion
Structures of Respiratory System • Inhaled air passes from pharynx larynx trachea right and left bronchi bronchioles terminal bronchioles respiratory bronchioles alveoli
Pharynx and Larynx • Air enters the trachea from the pharynx • Air must enter or leave trachea and lungs thru the glottis between the vocal folds • ventricular and vocal folds are part of the larynx (voice box)
Structure of Respiratory System • Respiratoryzone – region of gas exchange occurs only in respiratory bronchioles and the terminal alveoli sacs • Conductingzone – airways that conduct air to the respiratory zone
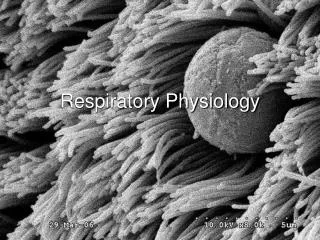
Lung Alveoli and Pulmonary Capillaries • Gas exchange occurs across the 300 million alveoli (60-80 m2 total surface area) • Alveolus – one cell-layer thick • Total ‘air-blood’ barrier only 2 thin cells across • Between lung air and blood: 1 alveolar cell and 1 endothelial cell
Alveoli • Polyhedral in shape – clustered at ends of respiratory bronchioles, like units of honeycomb • Air in 1 cluster can pass to others through pores • 2 types of alveolar cells • Type I: comprise 95 – 97% of total surface lung area • Primarily where gas exchange occurs • Diffusion distance between blood and air as little as 0.3 µm • Type II: secrete pulmonary surfactant and reabsorb Na+ and H2O • Prevents fluid buildup within the alveoli
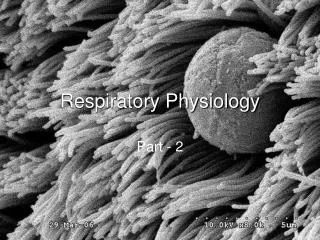
SEM of Lung Tissue • A small bronchile passes between many alveoli • Arrow – indicating an alveolar pore • air can pass from one cluster to another • Tensile strength of alveolar wall provided by fused basement membranes (collagen) of the capillaries and alveolar walls
Conducting Zone • Warms and humidifies inspired air – reaches respiratory zone at 37 °C • Mucus lining filters and cleans inspired air – mucous moved by cilia to be expectorated
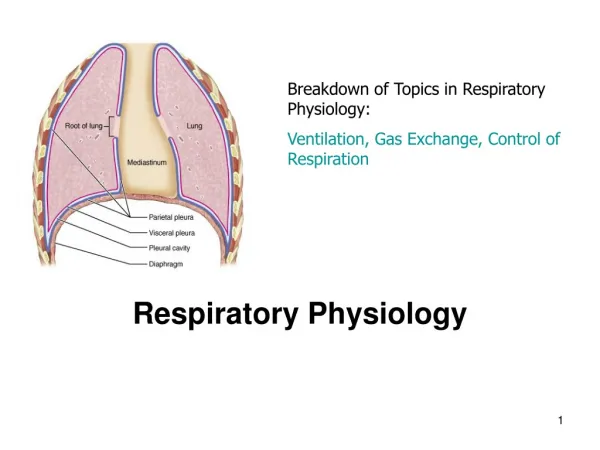
Thoracic Cavity • Created by the diaphragm – contains heart, large blood vessels, trachea, esophagus, thymus, and lungs • Abdominopelvic cavity below the diaphragm – contains liver, pancreas, GI tract, spleen, and genitourinary tract
Physical Aspects of Ventilation • Ventilation results from pressure differences induced by changes in lung volumes • Air moves from higher to lower pressure • Compliance, elasticity, and surface tension of lungs influence ease of ventilation
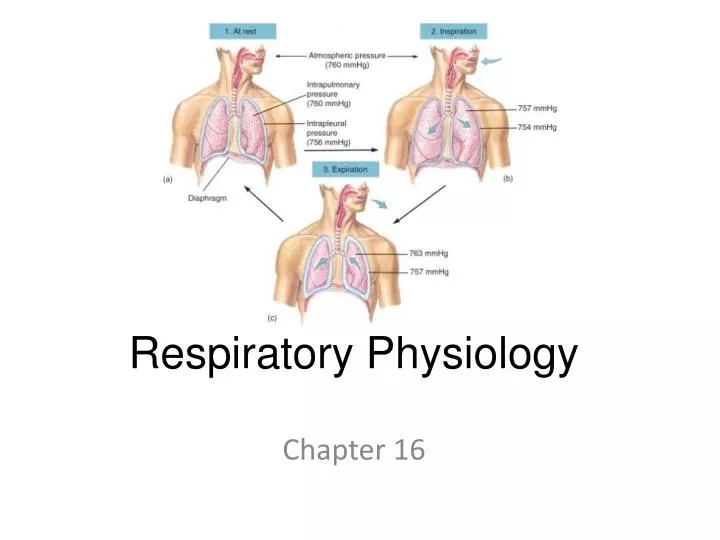
Intrapulmonary and Intrapleural Pressures • Visceral and parietal pleurae normally adhere to each other so that lungs remain in contact with chest walls • And expand and contract with thoracic cavity • Intrapleural space contains a thin layer of lubricating fluid
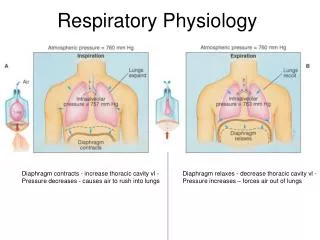
Intrapulmonary and Intrapleural Pressures • During inspiration, intrapulmonary pressureis about -3 mm Hg pressure; during expiration is about +3 mm Hg • Positive transmural pressure(intrapulmonary minus intrapleural pressure) keeps lungs inflated
Boyle’s Law (P = 1/V) • Implies that changes in intrapulmonary pressure occur as a result of changes in lung volume • Pressure of a given quantity of gas is inversely proportional to its volume • Increase in lung volume during inspiration decreases intrapulmonary pressure to subatmospheric levels • air therefore goes in • Decrease in lung volume raises intrapulmonary pressure above that of the atmosphere • Expelling air from the lungs • Changes in lung volume occur as a consequence of changes in thoracic volume
Physical Properties of the Lungs • In order for inspiration to occur lungs must be able to expand when stretched • Lung compliance – how easily lung expands with pressure • Lung compliance is defined as the change in lung volume per change in transmural pressure (V/P) • Compliance is reduced by factors that cause resistance to distension
Elasticity • For expiration to occur, lungs must get smaller when tension is released • Elasticity – tendency to return to initial size after distension • Due to high content of elastin proteins • Elastic tension increases during inspiration and is reduced by recoil during expiration
Surface Tension (ST) • And elasticity – forces that promote alveolar collapse and resist distension • Lungs secrete and absorb fluid (antagonistic processes), normally leave a very thin film of fluid on alveolar surface • Fluid absorption occurs by osmosis driven by Na+ active transport • Fluid secretion is driven by active transport of Cl- out of alveolar epithelial cells • This film causes ST because H20 molecules are attracted to other H2O molecules • ST acts to collapse alveoli; thus increasing pressure of air within alveoli
Surface Tension • Law of Laplace – states that pressure in alveolus is directly proportional to ST; and inversely to radius of alveoli • Thus, pressure in smaller alveoli would be greater than in larger alveoli, if ST were same in both • Greater pressure of smaller alveolus would cause it to its empty air into the larger one
Surfactant • Consists of phospholipids secreted by Type II alveolar cells • Lowers ST by getting between H2O molecules at the water-air interface • Reducing their ability to attract each other via hydrogen bonding • As a result the ST of thhe alveoli is negligible
Surfactant • Prevents ST from collapsing alveoli • Surfactant secretion begins in late fetal life • Premies are often born with insufficient surfactant = Respiratory Distress Syndrome or RDS • Have trouble inflating lungs • In adults, septic shock (fall in BP due to widespread vasodilation) as a result of a systemic infection • Inflammation increases capillry and alveolar permeability leading to accumulation of protein-rich fluid in the lungs • may cause acute respiratory distress syndrome(ARDS) which decreases compliance and surfactant secretion
Mechanics of Breathing • Pulmonary ventilation consists of inspiration (inhalation) and expiration (exhalation) • Accomplished by alternately increasing and decreasing volumes of thorax and lungs
Quiet Breathing • Inspiration occurs mainly because diaphragm contracts, increasing thoracic volume vertically • Parasternal and external intercostal contraction contributes a little by raising ribs • increasing thoracic volume laterally • Expiration is due to passive recoil
Deep Breathing • Inspiration involves contraction of extra muscles to elevate ribs: scalenes, pectoralis minor, and sternocleidomastoid • Expiration involves contraction of internal intercostals and abdominal muscles
Mechanics of Pulmonary Ventilation • During inspiration, intrapulmonary pressure is lower while • During expiration it is greater than atmospheric pressure
Pulmonary Function Tests • Spirometry – method that measures volumes of air moved during inspiration and expiration • Subject breathes in a closed system • Air is trapped within a light plastic bell floating in water • Bell moves up with exhalation and down with inhalation • Movements of the bell cause movement os a pen that traces a record of the breathing (spirogram) • Anatomical dead space is air in conducting zone where no gas exchange occurs
Pulmonary Function Tests • Tidal volume–amount of air expired/breath in quiet breathing • Vital capacity– amount of air that can be forcefully exhaled after a maximum inhalation = sum of inspiratory reserve, tidal volume, and expiratory reserve