Download
1 / 78
780 likes | 1k Views
Breakdown of Topics in Respiratory Physiology: Ventilation, Gas Exchange, Control of Respiration. Respiratory Physiology. Functions of the Respiratory System. Respiration Acid-base balance Enabling vocalization Defense against pathogens and foreign particles

E N D
Breakdown of Topics in Respiratory Physiology: Ventilation, Gas Exchange, Control of Respiration Respiratory Physiology
Functions of the Respiratory System • Respiration • Acid-base balance • Enabling vocalization • Defense against pathogens and foreign particles • Route for water and heat losses
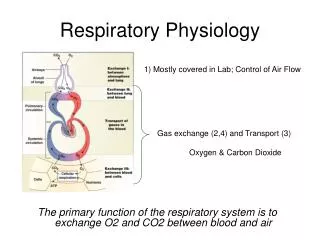
General Concepts of Respiration • Ventilate: bring the oxygen to the blood • Gas exchange: diffusion of gasses from alveoli into blood; then gasses go to/from erythrocytes; to /from Hemoglobin • O2 utilization: Mitochondria need the oxygen to make ATP (cellular respiration)
Ventilation • Ventilation is the process of bringing air into and out of the lungs. • Lungs are the only organs that do not have smooth muscle in them. They are just elastic tissue. • The lungs cannot inflate on their own. They need to be tethered to muscles in order to get volume changes, which causes pressure changes, which regulate air flow. • There are pressure gradients from the partial pressures of gasses. If the partial pressure of a gas is increased, the concentration of that gas increases, too. • Your lungs also contain millions of macrophages, so they are a good line of defense against pathogens. They also get rid of the dust and other debris that accumulates in the lungs. • They are also a route of heat and water loss. When you exhale, you lose water vapor and heat. 90% of the heat lost from your body is from exhaling.
Gas Exchange • In the lungs, oxygen moves into the blood, driven by pressure gradients, which are similar to concentration gradients. • Oxygen will diffuse down its concentration gradient (from the lungs, into the plasma, and into the cells) while CO2 moves down its concentration gradient (from the cells, into the plasma, and into the lungs). • These two gas exchanges are called external respiration.
Oxygen Utilization • When oxygen enters the cells, some of it enters the mitochondria, which uses oxygen as an electron acceptor (the mitochondria places hydrogen ions on the oxygen and turns it into water). This excess water leaves the cell and enters the tissues. • The removal of oxygen from the plasma and the addition of water in the tissues creates a driving force (known as the Starling principle) to continuously draw oxygen into the tissues, since the water in the tissues has diluted the number of particles there, and oxygen, as a particle, will be sucked into the tissues. • The gas exchange that occurs at the tissue capillary beds is called internal respiration. • The actual use of oxygen as a final electron acceptor(during a process called oxidative phosphorylation) is called cellular respiration.
General Concepts: Airway Anatomy Surface area 70 sq meters- each lung (size of a large lecture hall)! Barrier/ thickness to diffusion 0.2 microns
Carbon Monoxide • This is an odorless, colorless gas from incomplete burning of fuels. • Carbon monoxide binds to hemoglobin 200x more strongly than oxygen, so it drives the O2 from the hemoglobin, and attaches in its place and stays there. Carbon monoxide decreases the amount of oxygen that can be transported by hemoglobin • The person dies from suffocation; it makes the lips cherry red. • Cyanide poisoning kills in the same way, but the lips are blue (cyanosis).
CO2 Transport • When oxygen is on the hemoglobin molecule, it is called oxyhemoglobin. • Dissociation of oxyhemoglobin is when the oxygen is released and enters the tissues. • This dissociation increases as the pCO2 levels increase. • In other words, when the carbon dioxide levels rise, oxygen will jump off the hemoglobin and into the tissues. Therefore, the most effective stimulus to the respiratory center is an increase in pCO2. • The waste product of cellular respiration is carbon dioxide. • CO2 will then attach onto the hemoglobin and be taken to the lungs to be expelled.
CO2 Transport • CO2 is carried to the lungs on the hemoglobin, after the oxygen has left to enter the tissues. • The carbon dioxide reacts with water in the RBC to form carbonic acid, which then breaks apart into a hydrogen ion (which lowers blood pH) and a bicarbonate ion (which raises blood pH). CO2 + H2O H2CO3 H+ + HCO3- This reaction is reversible, and would go mainly to the right in the tissues and to the left in the lungs. CO2 is transported in the blood predominately in the form of bicarbonate. The number of H+ ions in the blood depends partly on the amount of CO2 in the blood. The more CO2 in the blood, the more H+ in the blood, which makes the blood acidic. If the blood is too acidic, bicarbonate ions are absorbed to raise the pH. If the blood is to alkaline, bicarbonate ions are excreted by the kidneys.
Respiratory System Contribution to pH Balance in the Blood • If a person has excess H+ ions in the blood (acidosis), they will breathe more rapidly. • If the person has an airway obstruction (such as asthma), they cannot exhale the excess CO2. • Because the H+ are building up, the carbonic acid will also build up, causing a drop in pH (acidosis) in the blood. • Enzymes in the body cannot work outside of their optimal pH range, so chemical reactions come to a halt. • Hyperventilation results in too little CO2 in the blood, so the person has a high pH (alkalosis), which also denatures enzymes.
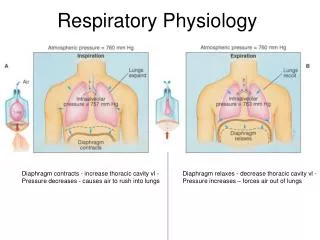
Control of Respiration • Changes in lung volume, and thus ventilation, are dependent upon the change in thoracic cavity volume. • Alterations in the space inside the thoracic cavity are the result mainly of the contraction of the diaphragm, intercostal muscles. • These muscles are innervated by neurons in the respiratory centers of the brain stem (medulla and pons).
Respiratory Centers: Medulla oblongata and Pons • Pons (Pneumotaxic Center) • decreases respiratory rate • Medulla • Dorsal respiratory group • Increases inspiration rate • Ventral Respiratory Group • Inactive during quiet respiration • Active during forced respiration Figure 41-1; Guyton & Hall
Chemoreceptors • Carbon Dioxide, Hydrogen Ions • Central chemosensitive area of medulla; senses levels of CO2 and H+ in CSF (both are acids) • Oxygen • Peripheral chemoreceptors; sense oxygen levels in blood • Aortic chemoreceptors (CN X) • Carotid chemoreceptors (CN IX)
Respiratory Chemoreceptors • In the cardiovascular lecture, we learned about baroreceptors detecting blood pressure in the aortic arch and carotid sinus. • The respiratory system has chemoreceptors in those areas, too. They function to detect the O2, CO2, and pH levels of the blood. • The medulla oblongata also has chemoreceptors that monitor pH. This information is sent to the other parts of the respiratory centers (pons and other areas in the medulla oblongata) to allow them to alter breathing rate to maintain proper blood pH.
Control of Respiration • Relaxed breathing only requires the diaphragm to contract for inspiration, and for the diaphragm to relax for expiration. • Forced breathing requires the diaphragm plus muscles that raise and lower the ribs (external intercostals for inspiration, internal intercostals for expiration). • The respiratory centers are most sensitive to the level of CO2 in the blood, rather than the levels of oxygen.
Control of Gas at Cellular Level • The flow of blood through capillaries is controlled by sphincters on the arterioles and capillary beds to adjust the amount of blood flowing to particular tissues. • Cells and tissues that are undergoing increased aerobic activity have less oxygen and more CO2, lower pH, and increased temperature. • When CO2 levels in the tissues are too high, the smooth muscle sphincters relax to allow more blood flow to increase gas exchange.
Ventilation Inspiration (inhalation) Expiration (exhalation) Normal inhalation, normal exhalation Forced inhalation, forced exhalation • Concepts: • Pressure gradient created by volume changes (Boyle’s Law) • Anatomy of lung and chest wall
Inhalation and Exhalation vs. Force • Ventilation requires ATP during inhalation, but normal exhalation does not require ATP. • Some people with respiratory problems need to work at exhalation as well by using skeletal muscle, and this means that they need to use more ATP. Lungs are not muscular structures. They need the skeletal muscles in the thoracic cage to change the thoracic volume, which changes the pressure gradients. • Air flows from high pressure to low pressure.
Boyle's Law P1V1=P2V2 • Pressure and volume are inversely related (if other variables are kept constant.) Boyle’s Law assumes normal circumstances, not a person who is in high altitude or who has variation in body temperature.
Air Pressure in Lungs • Every time a molecule strikes the wall of a container, it causes pressure. In a larger container with fewer molecules, it takes a while to strike the wall randomly, so there is less pressure. • The number of impacts on a container wall is the pressure. • The lungs must have a volume change to create a pressure change, which is required to have air move into and out of the lungs.
Air Pressure in Lungs • The diaphragm is the muscle that mostly contributes to the volume change. When it contracts, it pulls downward, and the volume of the thoracic cavity increases. • The external intercostals elevates the ribcage, giving the lungs more room, so they also increase the lung volume. • Those two muscles cause increased volume.
Air Pressure in Lungs • Because the lungs are tethered to the thoracic cavity, when your chest wall expands, your lungs expand with it. The lungs are stuck to the chest wall because the serous fluid in the pleural cavity makes the lungs stick to the chest wall like two pieces of wet glass stuck together. • When the lungs expand, their volume expands. That means there is less pressure in the lungs than there is in the outside air. Since air moves from high to low pressure, air flows into the lungs. • As air flows in, the alveoli expand, so the volume in each air sac expands, so the pressure in the alveoli lowers. Air in the conducting passages (bronchi) is at higher pressure, so it will move from high to low pressure areas. Therefore, air will move into the alveoli.
Air Pressure in Lungs • Air has weight; atmospheric pressure is 760 mmHg at sea level (much less weight and pressure at high altitudes). • Since air will flow from higher pressure to lower pressure areas, to get the air to flow into our lungs, we need to have a lower pressure in our lungs. • We can decrease the pressure in our lungs by expanding the volume. As we expand the volume of our thoracic cavity (taking a breath), the pressure in the lungs drops, and air flows into the lungs. • It is a small pressure difference, but it is enough to get 500 ml of air to come into your lungs. • At higher altitudes, even though the amount of oxygen is the same (21%) there is less air pressure. At 8,000 feet in elevation, there is ¼ less pressure. This makes it harder to breathe. • When you exhale, you simply relax the muscles, and if the lungs are not being pulled open any more, the elastic tissue there will recoil, making the lung volume smaller, so the pressure there increases.
Lung Compliance • Lung Compliance is how much the lung volume changes when the pressure changes. • Compliance can be considered the opposite of stiffness. • A low lung compliance (increase in stiffness) would mean that the lungs would need a greater than average change in pressure to change the volume of the lungs. Instead of needing only 10 mmHg pressure difference between the outside air and the lungs, would now need a 20 mm difference. • A high lung compliance would indicate that little pressure difference is needed to change the volume of the lungs. • More energy is required to breathe in a person with low lung compliance. Persons with low lung compliance due to disease therefore tend to take shallow breaths and breathe more frequently.
Gases move down pressure gradients P atm = 760 torr Flow Rule: Patm – Palv Resistance How are the pressure gradients changed? According to Boyle’s law we will need to create volume changes! PROBLEM! THE LUNGS ARE NOT MUSCULAR STRUCTURES! p alveolar = 758 torr Air moves from high to low pressure
Air Pressure in Lungs • We are looking at two types of air pressures: atmospheric pressure, and the pressure of air deep in the lungs, called the alveolar (pulmonary) pressure. • As long as there is a difference in pressure between these two, there will be a pressure gradient, and air will flow. • If they equal each other (such as during a punctured lung, called a pneumothorax), air will not flow.
Air Pressure in Lungs • Take a breath in and stop. Enough air has come in now so that the air pressure in the alveoli equals the atmosphere, so you no longer get more air flowing in. • When you relax, the lungs recoil, air comes out, and when the two pressures equal each other, air stops flowing out. • You will get zero pressure differences upon maximum inhalation and exhalation.
Oxygen-Hbg Dissociation Curve • X-axis is partial pressure of oxygen (pO2) • Y-axis is saturation of Hgb with O2 • The partial pressures of respiratory gases found in arterial blood correspond most closely to those partial pressures found in the alveoli.
Oxygen-Hbg Dissociation Curve • Hgb in the blood leaving the lungs is about 98% saturated with O2. • This graph demonstrates that 98% of Hbg is still saturated when pO2 is only 70 mm (when it first arrives in the tissues). • By the time pO2 reaches 100mm (in the lungs), Hbg is already 100% saturated.
Significance • In the lungs, pO2 is 100 mm Hg. Hemoglobin is still 100% saturated at this pO2 level. • In the body cells, pO2 is 40 mm Hg. Hemoglobin is still about 75% saturated at this low pO2 level. • The difference of 25% saturation means that hemoglobin gives up only about 25% of its O2 to body cells as it passes by.
Left shift CAUSE: pH increased CO2 decreased Temperature decreased
Right shift CAUSE: pH decreased CO2 increased Prostaglandin release (fever)
Shifts • A left shift will increase oxygen's affinity for hemoglobin. • In a left shift condition (alkalosis or hypothermia) oxygen will have a higher affinity for hemoglobin (it won’t leave!). • This can result in tissue hypoxia even when there is sufficient oxygen in the blood. • A right shift decreases oxygen's affinity for hemoglobin. • In a right shift (acidosis or fever) oxygen has a lower affinity for hemoglobin. Blood will release oxygen more readily. • This means more O2 will be released to the cells, but it also means less oxygen will be carried from the lungs in the first place.
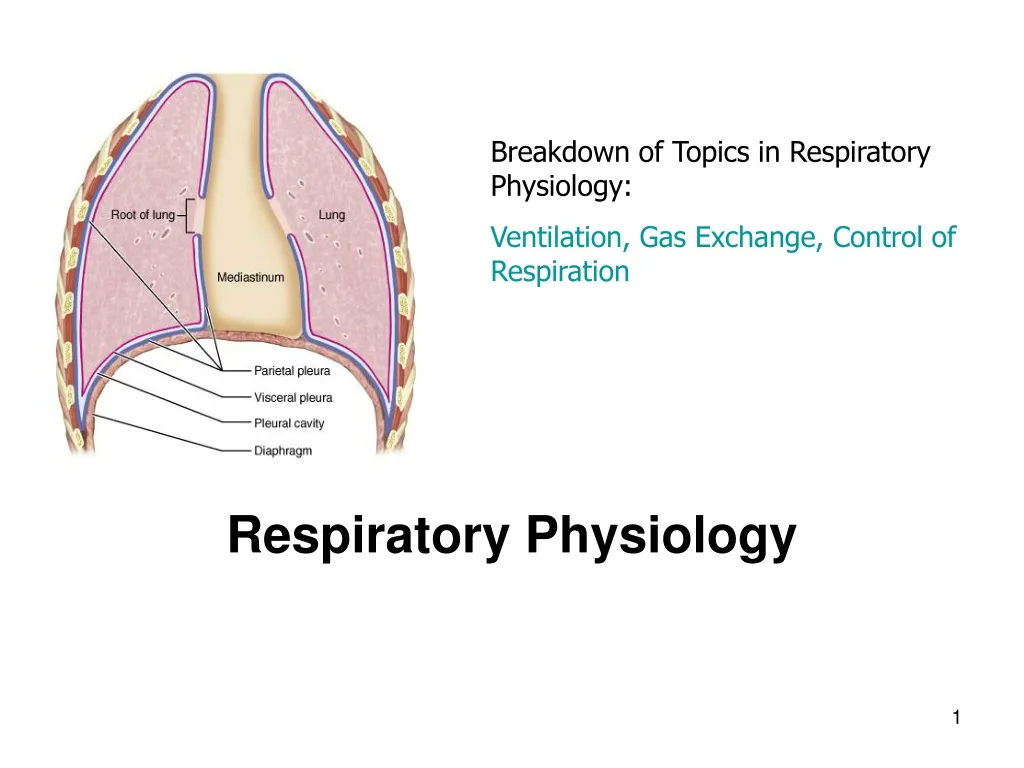
Vacuum in Lungs • There is another anatomical structure you need to remember: the plural cavity. Each lung is surrounded by a parietal and visceral serousal membrane. • The serousal cells make a lubricating fluid so the lungs don’t rub against the thoracic cavity, causing heat generation, which can denature proteins. • This fluid has cohesive properties. If you put two pieces of wet glass together, you have to use more force to pull them apart than if they were dry. You have to break the vacuum.
Vacuum in Lungs • The surface of the lungs are tightly stuck to the surface of the thoracic wall. • If they are disengaged, they will recoil like deflated balloons. • If the vacuum in the pleural cavity is broken, the lung will collapse. • They need to be reinflated by the administration of oxygen.
Diaphragm Mechanics of Ventilation • Normal Inspiration • Is an active process (It’s work! It uses ATP) • Contract Diaphragm and it moves inferiorly to increase thoracic volume -60-75% of volume change • Contract external intercostals • Forced Inspiration • Accessory muscles needed • Sternocleidomastoid • Scalenes • Serratus anterior • Others (erector spinae)
When the chest wall moves, so do the lungs! Why are the lungs right up against the chest wall? • Pleural Space or Cavity • a vacuum (contains no air) • pleural fluid (water) has surface tension Result? Lung moves with the chest wall Lungs are not muscular organs, they cannot actively move. They move with the chest wall.
What happens if the lung dissociates from the chest wall? • Pneumothorax: air in the pleural cavity • Hemothorax: blood in the pleural cavity • How? • Injury (Gun shot, stabbing) • Spontaneous (tissue erosion, disease lung) • Bleeding wound • Chest wall recoils outward (barrel chest) • Lung recoils inward (atelectasis = alveolar, lung collapse)
Mechanics of Ventilation • Normal Expiration- • A Passive process • Simply relax the muscles of inspiration • Rely on the elastic properties of lung (like a balloon deflating on its own) • Forced Expiration • Relax muscles of inhalation AND • Contract internal intercostals • Contract Abdominal muscles • Internal and external obliques • Transverse abdominis • Rectus abdominis
Emphysema • COPD (chronic obstructive pulmonary disease) is emphysema plus chronic bronchitis. • Emphysema is generally caused by smoking. • The alveoli have broken, leaving spaces where gas exchange cannot take place. • Compliance decreases, so It is difficult to expel the air in the lungs. • Each inhalation is a forced inspiration also. • When the ribs are continually raised with each breath, they eventually remain in the upright position, causing a barrel chest.
Exhalation Problem: COPD • Normal exhalation is passive, requires no ATP. But forced expiration (such as emphysema patient) recruits abdominal muscles. The muscles enlarge with time, creating a barrel-shaped chest, typical of emphysema patients and COPD.
COPD • In everyone, the midsized bronchioles do not have cartilage rings to hold them open, and during exhalation, the sides of the bronchioles collapse and touch each other. • If there is not enough surfactant, they stick to each other with greater strength (like two wet pieces of glass), and the person has to forcefully exhale with each breath to overcome the cohesiveness of the fluid. • Surfactant is like adding soap to the fluid so the surfaces come apart easier.
Exhalation • Giving oxygen in high concentration helps get air into their lungs, but it reduces the drive for them to breathe. CO2 is a powerful driving force for ventilation. When a person has COPD, they have less CO2, and oxygen becomes the driving force. • If we give them oxygen, the drive for them to breathe becomes diminished. They eventually wind up on a positive pressure ventilator, but the disease progresses, and they die from suffocation. • A continuous positive airway pressure machine is called a CPAP machine.
Both the Lung and Chest Wall are Elastic • Both lung and chest wall have the tendency to recoil • What is recoil? Tendency to snap back to resting position (like a stretched rubber band recoils when youlet go of one end) The chest wall recoils outward (springs out) The lung recoils inward (ie. it collapses!)
expiration inspiration Palv=0 Palv (mmHg) Palv=+1 Palv=0 Palv=0 Palv= -1 0.5 Breath vol. (L) • Increase in lung volume decreases intra-alveolar pressure (we now have a pressure gradient) = air goes in. • Decrease in lung volume raises intra-alveolar pressure above atmosphere = air goes out. When the pressure at the alveoli are at 0 (no difference between their pressure and atmospheric pressure), no air flows in or out of the lungs.
Pressures Patm and Palv create the pressure gradient that drives ventilation Atmospheric Pressures (Patm)- pressure of the outside air (760mmHg=760 torr = 1 atm). Intra-alveolar pressure (Palv) pressure within the alveoli of the lungs. Equal to Patm (0mmHg) at rest, but varies during phases of ventilation. Intra-pleural pressure – (Pip) pressure in the intra-pleural space. • Pressure is negative because of thelack of air in the intrapleural space, lymph drainage, and opposing forces of lung and chest wall.
Air Flow • If atmospheric pressure is greater than alveolar pressure, air flows into the lungs. • If atmospheric pressure is less than alveolar pressure, air flows out of the lungs. • Transpulmonary pressure is the difference between the alveolar and intra-pleural pressures.
Positive Pressure breathing Negative Pressure breathing