Download
1 / 45
830 likes | 1.55k Views
Respiratory Physiology. Chapter 16. Chapter 16 Outline The Respiratory System Physical Aspects of Ventilation Mechanics of Breathing Gas Exchange in the Lungs Regulation of Breathing Hemoglobin and Oxygen Transport CO 2 Transport Acid-Base Balance of the Blood

E N D
Respiratory Physiology Chapter 16
Chapter 16 Outline • The Respiratory System • Physical Aspects of Ventilation • Mechanics of Breathing • Gas Exchange in the Lungs • Regulation of Breathing • Hemoglobin and Oxygen Transport • CO2 Transport • Acid-Base Balance of the Blood • The Effect of Exercise and High Altitude on Respiratory Function 16-2
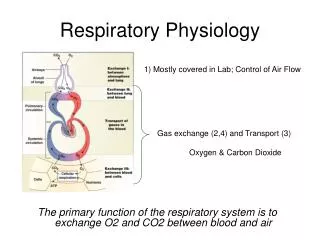
Respiration • Encompasses 3 related functions: • Ventilation • gas exchange • O2 utilization (cellular respiration) • Ventilation moves air in and out of lungsfor gas exchange with blood (external respiration) • Gas exchange between blood and tissues, and O2 use by tissues is internal respiration • Gas exchange is passive via diffusion 16-3
Structure of Respiratory System • Air passes from mouth to trachea to right and leftbronchi to bronchioles to terminal bronchioles to respiratorybronchioles to alveoli • Gas exchange occurs only in respiratory bronchioles and alveoli (= respiratory zone) • All other structures constitute the conducting zone • Are polyhedral in shape and clustered at ends of respiratory bronchioles, like units of honeycomb
Structure of Respiratory System • Gas exchange occurs across the 300 million alveoli (60-80 m2 total surface area) • Only 2 thin cells are between lung air and blood: 1 alveolar and 1 endothelial cell
Conducting Zone • Warms and humidifies inspired air • Mucus lining filters and cleans inspired air • Mucus moved by cilia to be expectorated
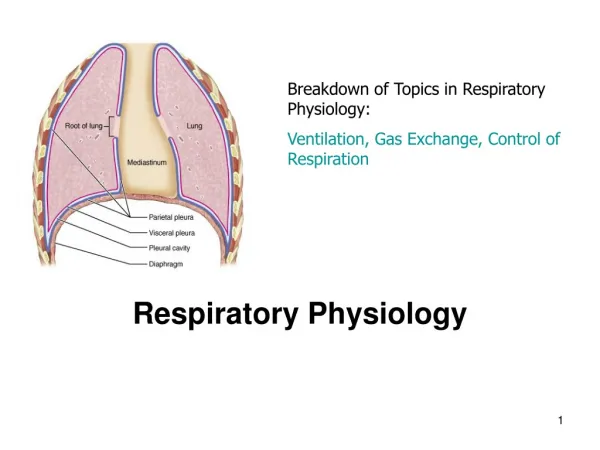
Thoracic Cavity • Is created by the diaphragm, a dome-shaped sheet of skeletal muscle • Contains heart, large blood vessels, trachea, esophagus, thymus, and lungs • Below diaphragm is abdominopelvic cavity • Contains liver, pancreas, GI tract, spleen, and genitourinary tract
Thoracic Cavity • Intrapleural space is thin fluid layer between visceral pleura covering lungs and parietal pleura lining thoracic cavity walls
Physical Aspects of Ventilation • Ventilation results from pressure differences induced by changes in lung volumes • Air moves from higher to lower pressure • Ease of Ventilation influence by: • Compliance • Elasticity • Surface tension
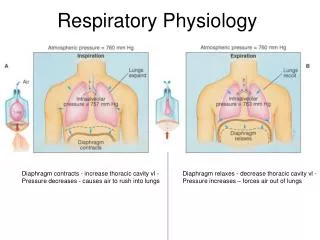
Intrapulmonary and Intrapleural Pressures • Visceral and parietal pleurae normally adhere to each other so that lungs remain in contact with chest walls • And expand and contract with thoracic cavity • Intrapleural space contains a thin layer of lubricating fluid • During inspiration, intrapulmonary pressure is about -3 mm Hg pressure; during expiration is about +3 mm Hg • Positive transmural pressure/transpulmonary (intrapulmonary minus intrapleural pressure) keeps lungs inflated
Boyle’s Law (P = 1/V) • Implies that changes in intrapulmonary pressure occur as a result of changes in lung volume • Pressure of gas is inversely proportional to volume • Increase in lung volume decreases intrapulmonary pressure to subatmospheric levels; air goes in • Decrease in lung volume raises intrapulmonary pressure above that of the atmosphere; air expelled from lungs 16-17
Compliance • Is how easily lung expands with pressure • Or change in lung volume per change in transmural pressure (V/P) • Is reduced by factors that cause resistance to distension – such as pulmonary fibrosis
Elasticity • Is tendency to return to initial size after distension • Due to high content of elastin proteins • Elastic tension increases during inspiration and is reduced by recoil during expiration • Factors that cause reduced elasticity – such as Emphysema
Surface Tension (ST) • ST and elasticity are forces that promote alveolar collapse and resist distension • Lungs secrete and absorb fluid, normally leaving a thin film of fluid on alveolar surface • Fluid absorption occurs by osmosis driven by Na+ active transport • Fluid secretion is driven by active transport of Cl- out of alveolar epithelial cells • This film causes ST because H20 molecules are attracted to other H2O molecules • ST acts to collapse alveoli; thus inc. pressure of air within alveoli 16-20
Surfactant • Consists of phospholipids secreted by Type II alveolar cells • Lowers ST by getting between H2O molecules, reducing their ability to attract each other via hydrogen bonding
Mechanics of Breathing 16-24
Mechanics of Breathing • Pulmonary ventilation consists of inspiration (= inhalation) and expiration (= exhalation) • Accomplished by alternately increasing and decreasing volumes of thorax and lungs 16-25
Quiet Breathing • Inspiration occurs mainly because diaphragm contracts, increasing thoracic volume vertically • Parasternal and external intercostal contraction contributes a little by raising ribs, increasing thoracic volume laterally • Expiration is due to passive recoil 16-26
Deep Breathing • Inspiration involves contraction of extra muscles to elevate ribs: scalenes, pectoralis minor, and sternocleidomastoid muscles • Expiration involves contraction of internal intercostals and abdominal muscles 16-27
Pulmonary Function Tests • Assessed clinically by spirometry, a method that measures volumes of air moved during inspiration and expiration • Anatomical dead space is air in conducting zone where no gas exchange occurs 16-29
Pulmonary Function Tests • Tidal volume is amount of air expired/breath in quiet breathing • Vital capacity is amount of air that can be forcefully exhaled after a maximum inhalation • = sum of inspiratory reserve, tidal volume, and expiratory reserve
Partial Pressure of Gases • Partial pressure is pressure that a particular gas in a mixture exerts independently • Dalton’s Law states that total pressure of a gas mixture is the sum of partial pressures of each gas in mixture • Atmospheric pressure at sea level is 760 mm Hg • PATM = PN2 + PO2 + PCO2 + PH2O = 760 mm Hg
Gas Exchange in Lungs • Is facilitated by enormous surface area of alveoli, short diffusion distance between alveolar air and capillaries, and tremendous density of capillaries 16-43
Blood PO2 and PCO2 Measurements • Provide good index of lung function • At normal arterial blood has about PO2= 100mmHg • PO2 = 40mmHg in systemic veins • PCO2 = 46mmHg in systemic veins
Pulmonary Circulation • Rate of blood flow through pulmonary circuit equals flow through systemic circulation • But is pumped at lower pressure (about 15 mm Hg) • Pulmonary vascular resistance is low • Low pressure produces less net filtration than in systemic capillaries • Avoids pulmonary edema • Pulmonary arterioles constrict where alveolar PO2 is low and dilate where high • This matches ventilation to perfusion 16-46
Lung Ventilation/Perfusion Ratios • Normally, alveoli at apex of lungs are underperfused and overventilated • Alveoli at base are overperfused and underventilated 16-47
Regulation of Breathing 16-50
Brain Stem Respiratory Centers • Automatic breathing is generated by a rhythmicity center in medulla oblongata • Consists of inspiratory neurons that drive inspiration and expiratory neurons that inhibit inspiratory neurons • Their activity varies in a reciprocal way and may be due to pacemaker neurons 16-51
Brain Stem Respiratory Centers • Inspiratory neurons stimulate spinal motor neurons that innervate respiratory muscles • Expiration is passive and occurs when inspiratory neurons are inhibited
Pons Respiratory Centers • Activities of medullary rhythmicity center are influenced by centers in pons • Apneustic center promotes inspiration by stimulating inspiratory neurons in medulla • Pneumotaxic center antagonizes apneustic center, inhibiting inspiration
Chemoreceptors • Automatic breathing is influenced by activity of chemoreceptors that monitor blood PCO2, PO2, and pH • Central chemoreceptors are in medulla • Peripheral chemoreceptors are in large arteries near heart (aortic bodies) and in carotids (carotid bodies)
Effects of Blood PCO2 and pH on Ventilation • Chemoreceptors modify ventilation to maintain normal CO2, O2, and pH levels • PCO2 is most crucial because of its effects on blood pH • H2O + CO2 H2CO3 H+ + HCO3- • Hyperventilation causes low CO2 (hypocapnia) • Hypoventilation causes high CO2 (hypercapnia)
Effects of Blood PCO2 and pH on Ventilation • Brain chemoreceptors are responsible for greatest effects on ventilation • H+ can't cross BBB but CO2 can, which is why it is monitored and has greatest effects • Rate and depth of ventilation adjusted to maintain arterial PCO2 of ~40 mm Hg • Peripheral chemoreceptors do not respond to PCO2, only to H+ levels
Effects of Blood PCO2 and pH on Ventilation A rise in blood CO2 inc. the H+ concentration (lowers pH) of CSF and thereby stim. chemoreceptor neurons in the medulla oblongata.
Effects of Blood PO2 on Ventilation • Low blood PO2 (hypoxemia) has little effect on ventilation • Does influence chemoreceptor sensitivity to PCO2 • PO2 has to fall to about half normal before ventilation is significantly affected • Emphysema blunts chemoreceptor response to PCO2 • Oftentimes ventilation is stimulated by hypoxic drive rather than PCO2 16-60