Download
1 / 14
140 likes | 346 Views
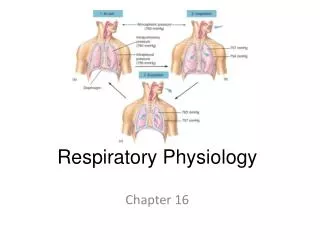
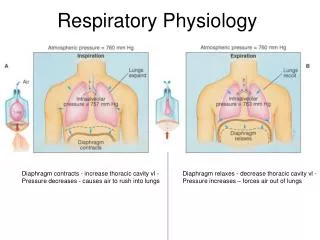
Respiratory Physiology. Mechanics. Chest – expands outwards Lungs – collapse Alveoli – act as bubbles (liquid-air interface) P = (2 x surface tension)/radius Collapse more likely when surface tension increases or alveolar size decrease

E N D
Mechanics • Chest – expands outwards • Lungs – collapse • Alveoli – act as bubbles (liquid-air interface) • P = (2 x surface tension)/radius • Collapse more likely when surface tension increases or alveolar size decrease • Surfactant made from Type II pneumocytes decreases surface tension • Compliance – change in volume/change in distending pressure – can be measured for lung, chest wall • Measures elastic recoil • Total system compliance = 1/Ctotal = 1/Cw +1/CL
Volumes • FRC – volume at end of normal exhalation (Vt) • Inward recoil of lung approx equal to outward recoil of chest – elastic properties determine normal breathing – can be measure by nitrogen washout, helium wash-in, or body plethysmography • Factors affecting FRC: 1) habitus – directly proportional to height. Obesity decreases frc d/t dec chest compliance. • 2) Sex – females 10% less; 3) posture – decreases from upright to sitting to prone – d/t dec chest compliance from abd contents – Greatest change from 0-60 deg of inclination • 4)lung dz, 5) diaphragmatic tone • Decreases 15-20% with induction of anesthesia • Vt – normal breath • IRV – max inspiration above Vt; ERV – max exp below Vt • RV – volume remaining after max exp • TLC – RV+ERV+Vt+IRV • FRC – RV + ERV • VC – max volume expired after max inspiration – dependent on habitus, respiratory muscle strength, chest-lung compliance
Closing capacity – volume at which small airways begin to close • small airways depend on elastic recoil of surrounding tissues for patency – dependent on lung volume, especially at bases • Normally below FRC, but rises with age, leading to shunts (perfused but not ventilated), probably responsible for age-related decline in PaO2 • At avg 44, FRC=CC while supine, at 66, CC = or > FRC while upright
Airway Resistance Flow = pressure gradient/Raw Raw = (8 x length x viscosity)/(pi x radius^4) Turbulent flow – high gas flows, branching points – sensitive to airway caliber Reynolds number <1000 – laminar flow = (linear velocity x diameter x gas density)/gas viscosity Airway resistance highest in medium airways
FVC Forced expiration of VC to evaluate airway resistance FEV1 – forced expiratory volume in 1 sec FEV1/FVC - proportional to degree of obstruction – normally >80% FEV25-75% - less effort dependent
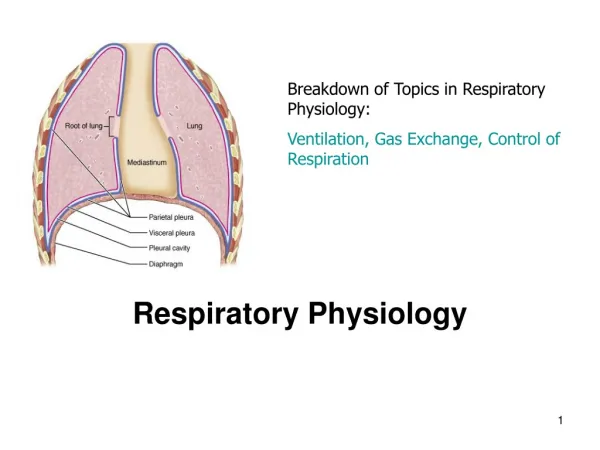
Dead space – anatomic + alveolar • Approx 150cc in adults (2cc/kg) • Shunt vs Dead Space • Hypoxic pulmonary vasoconstriction – shunts blood away from underventilated areas, preventing hypoxemia(alveolar hypoxia more powerful stimulus than pulmonary arterial hypoxia) • Volatile agents can inhibit this in high doses • Hypercapnia and acidosis – constrict • Hypocapnia – pulmonary vasodilation
Alveolar Oxygen Tension • PAO2 = ((Pb – PH20) x FiO2) – (PaCO2/RQ) • Pb – barometric pressure – 760 • PH20 – vapor pressure of water 47 mmHg at 37 deg • RQ – usually 0.8 • (760-47) x .21 = 149.7
Calculate PAO2 for RA, PCO2 of 40 • PCO2 of 75, RA • PAO2 for PCO2 of 40, FiO2 100% • PCO2 of 40, FiO2 50%
Binding of first 3 O2 to Hgb greatly facilitates binding of last O2 – responsible for linear portion of curve • Rightward shift – decreases O2 affinity, increases availability • Leftward shift – opposite • 2,3 DPG – byproduct of glycolysis, builds up in anaerobic metabolism • Important points on O2 curve: P50 – 26.6 mmHG PO2 • SpO2 90% - 60mmHg O2; SpO2 80% - 50mmHg O2; SpO2 70% - 40mmHg O2
Carbon Monoxide – higher affinity for Hgb, keeps SpO2 at 100% • Methemoglobin – also displaces O2, sats 85%-90%; treatment is methylene blue • Hurricane Spray • Oxygen Carrying Capacity • CaO2 = (Hb x 1.36 x SpO2/100) + (PaO2 x .003)
Control of Breathing • Central Receptors – medulla – responds to changes in CSF H+ concentration • Regulates PCO2, BBB permeable to dissolved Co2, not bicarb • Increase in H+ concentration increases ventilation to a point (CO2 narcosis) • Peripheral Receptors – carotid, aortic bodies • Carotid bodies – main receptors – sensitive to PaO2, PaCO2, pH, arterial perfusion pressure (most sensitive to PO2 – activate when PO2<50) • Communicate with central respiratory centers via glossopharyngeal nerves • Also stimulated by cyanide, doxpram, large doses of nicotine • Dopaminergic neurons – ventilatory response abolished by anti-dopaminergic drugs, b/l carotid surgery • Lung Receptors – transmitted by vagus • Stretch receptors in bronchial smooth muscle – inhibit inspiration when lung volumes high; shorten exhalation when volumes low • Irritant receptors – in mucosa – noxious stimuli – increases respiratory rate, bronchoconstriction, coughing • J receptors – interstitial space – induce dyspnea in response to expansion of interstitial space volume and chemical mediators after tissue damage