Download
1 / 30
300 likes | 311 Views
Learn about leukemias, malignancies involving abnormal cell proliferation in bone marrow, through this comprehensive guide. Discover the classification, etiology, and clinical features of acute and chronic leukemias.

E N D
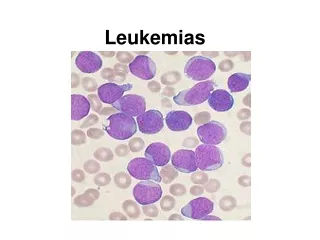
Leukemias are malignancies of hemtopoietic cells or tissues in which there is abnormal proliferation of hemopoietic cells with infiltration of bone marrow and lymphatic tissues ETIOLOGY: • Molecular biology of leukemogenesis- oncogenes • Abnormalities of the chromosomes- translocation deletions • Radiation • Chemicals • Viruses • Genetic factors-Down syndrome
CLASSIFICATION • LYMPHOID • ACUTE LYMPHOID LEUKEMIA (ALL) • CHRONIC LYMPHOID LEUKEMIA (CLL) • MYELOID • ACUTE MYELOID LEUKEMIA (AML) • CHRONIC MYELOID LEUKEMIA (CML)
ACUTE MYELOID LEUKEMIA
AML -NOT OTHERWISE CLASSIFIED MORPHOLOGIC CLASSIFICATION
MYELOBLAST WITH AUER ROD
NORMOBLASTS MYELOBLAST
AML-M4 AML-M5 AML-M6 MEGAKARYOBLASTS
CLINICAL FEATURES OF ACUTE LEUKEMIA: • COMMON • Anemia • Fever • Malaise • Hemorrhages, bruising and petechiae • LESS COMMON: • Infections of mouth and pharynx • Pains in bones and joints • URTI (children) • Superficial lymph node enlargement (children in ALL) • OCCASIONAL: • Abdominal pain • Skin rashes • Gum hypertrophy • Mediastinal obstruction
CLINICAL FEATURES DUE TO ORGAN INFILTRATION: • Tender bones • Superficial lymphadenopathy (ALL) • Splenomegaly, hepatomegaly (ALL) • Gum hypertrophy and infiltration, rectal ulceration and skin involvement (AML- myelomonocytic and andmonocytic type) • Meningeal syndrome (ALL) • Testicular swelling and mediastinal compression (ALL)
BLOOD PICTURE: • Normocytic and normochromicanemia • Total WBC count may be increased upto 500 x 10 /L • Thrombocytopenia • Peripheral blood smear- myeloblasts, promyelocytes, myelocytes , metamyelocytes, agranular neutrophils, stab cells, myelomonocytes and normoblasts • Bone marrow- hypercellular with plenty of blast cells (>75% of the marrow cell population) THERE SHOULD BE AT LEAST 30% BLASTS IN BONE MARROW (FAB ) 20% BLASTS IN BONE MARROW (WHO) 6. Tests for DIC will be positive in Promyelocyticleukemia
3. CYTOCHEMISTRY • Myeloperoxidase- positive in immuture myeloid cells containing granules and auer rods but negative in M0 myeloblasts • Sudan black- positive in immature cells in AML • Non specific esterase (NSE)- positive in monocytic series (M4 and M5) • Periodic acid Schiff (PAS)- positive in immature lymphoid cells and in erythroleukaemia (M6) • Acid phosphatase – focal positive in leukaemic blasts in ALL and diffuse reaction in monocytic cells (M4 and M5)
MYELOBLAST (MYELOPEROXIDASE POSITIVE)
4. IMMUNOPHENOTYPING • AML cells express CD13 and CD33 antigens • M5 shows CD41 and CD42 positivity • ALL is positive for CD10, CD19 in Pre B ALL (90%); B cell ALL (50%); • ALL T cell type are positive for CD1,CD2, CD5, CD7 5. OTHER INVESTIGATIONS • Serum muramidase- elevated in M4 and M5 AML • Serum uric acid- frequently elevated
COURSE AND PROGNOSIS IN AML: • GOOD PROGNOSIS • Age <40 year • M2,M3 and M4 types • Blast cells with Auer rods • Total WBC <25,000/cumm • Tranlocation and inversion • Leukemia without preceding Myelodysplastic syndrome (MDS) • BAD PROGNOSIS: • Age<2 years and >55 years • M0,M6,M7 types • Total WBC >100,000/cumm • Deletions • Leukemia with preceding MDS
ALL is the commonest leukemia seen in childhood • The predominant cell seen in ALL is LYMPHOBLAST • Lymphoblast has coarse nuclear chromatin and 1-2 nucleoli, high nucleus:cytoplasmic ratio (N:C), stain positve for PAS (periodic acid Schiff) and TdT (terminal deoxynucleotidyltransferase)
LYMPHOBLASTS (ALL)
MYELOBLASTS LYMPHOBLASTS
FAB CLASSIFICATION OF ALL • L1 ALL • Commonest type • Best prognosis • Lymphoblasts have coarse chromatin with small nucleoli and scanty cytoplasm • L2 ALL • Lymphoblasts have heterogenous chromatin with 1-2 nucleoli, moderate cytoplasm with few vacuoles • L3 ALL • Rare and worst prognosis • Homogenous chromatin with 1-2 prominent nucleoli, abundant cytoplasm and vacolues positive for Oil O Red
WHO IMMUNOLOGICAL CLASSIFICATION OF ALL • B CELL • More common • CD19 and Cd20 positive • Associated with pancytopenia • T CELL • Less common • CD1, CD2, CD7 positive • Associated with mediastinal mass, lympadenopathy and splenomegaly
CLINICAL FEATURES: • Same as AML • With lymphadenopathy, hepatsplenomegaly BLOOD PICTURE: • Elevated total WBC count upto 500,000/cum • Anemia, neutropenia • Thrombocytopenia • Lymphoblasts >30% in bone marrow BIOCHEMICAL CHANGES: • Elevated uric acid, LDH levels • Elevated serum phosphate levels • Hypocalcemia
PROGNOSIS IN ALL GOOD PROGNOSIS • Age 2-8 years • Females • L1 type • Pre-B cell • Absence of mediastinal mass • Hyperdiploidy or translocations BAD PROGNOSIS • Age < 2 year , >10 years • Male • L2 and L3 type • Pre T cell • Mediastinal mass • Ph chromosome