Download
1 / 60
610 likes | 875 Views
ALL Prognostic Factors. WHO-Classification 2008. B-lymphoblastic Leukemia/Lymphoma immunologic: Pro-B-, common-, Prä-B-ALL cytogenetic/molecular marker: t(9;22)(q34;q11.2) BCR-ABL1 t(4;11)(variabel;11q23)/ALL1-AF4

E N D
WHO-Classification 2008 • B-lymphoblastic Leukemia/Lymphoma immunologic: Pro-B-, common-, Prä-B-ALL cytogenetic/molecular marker: t(9;22)(q34;q11.2) BCR-ABL1 t(4;11)(variabel;11q23)/ALL1-AF4 t(12,21)(p13;q23)/TEL-AML1 • T-lymphoblastic Leukemia/Lymphoma immunologic: early-, cortical (thymic)-, mature T-ALL cytogenetic/molecular marker: t(10;14)(q24;q11) t(1;14)(p32,q11), t(11;14)(p15,q11) • Mature B-Cell Lekemia/Lymphoma Burkitt-ALL/NHL: t(8;14)/c-myc IgH Burkitt-NHL plasmacellular Differentiation Burkitt-Like-ALL/NHL
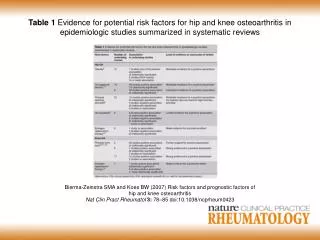
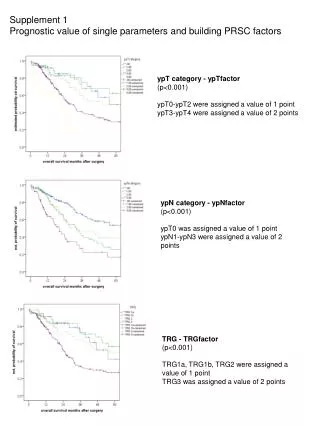
Biology of Disease: Cytogenetics *Hierarchical/mutually exclusive classification. †≥ 5 chromosomal abnormalities and no established structural abnormality/ploidy subgroup. Moorman AV, et al. Blood. 2007;109:3189-3197
ALL: Riskgroups (GMALL-Study) (1) • Standardrisk (SR): all Criteria are fullfilled • CR in less than 3 Weeks (Day 24) • WBC < 30 000/µl for B-Precursor-ALL • no Pre-T- or Pro-B-ALL • no t(9;22)/BCR-ABL-positive ALL • no t(4;11)/ALL1-AF4-positive ALL
ALL: Risikgroups (GMALL-Study) (2) • II. Highrisk (HR): only one Criteria is fullfilled • CR later than 3 Wochen (Day 24) • WBC > 30 000/µl for B-Precursor ALL • Pro-B, eraly-T • t(4;11)/ALL1-AF4-positive ALL • Very High Risk (VHR) • t(9;22)/BCR-ABL-positive ALL
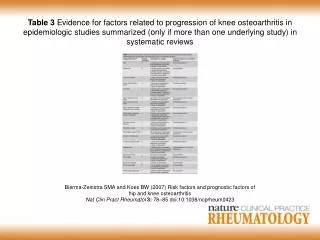
Outcome of Adult ALL Patients according to subgroups *Pooled data from published studies.**Depends on T-ALL subtype.***Depending on protocal and subtype.****Including allogeneic SCT.
Survival in ALL Has Improved in All Age Groups Except the Oldest Patients *Point estimates. Blood. Pulte D, et al. Blood. 2009;113:1408-1411
Acute LymphoblasticLeukemiaTherapy Backbone Induction Consolidation CNS Prophylaxis Reinduction Maintanance
1961 EFS Outcome by RER Groups Probability Log rank p = .001 5 Yr EFSRHR Augmented BFM 81.0% Baseline Standard BFM 70.2% 1.54 Years Followed Seibel et al, 2008
Outcome Comparison of Adolescent/Young Adults with ALL on Pediatric vs. Adult Clinical Trials
GMALL Study 07/2003 PEG-Asparaginase Intensification Stratification I According to risk factors Stratification II According to MRD HD-MTX ASP MRD NR SR End of therapy 6 MP HD-MTX ASP VM26 ARAC CYCLO ARAC HD-MTX ASP KI MRD HR Induction Reind. IFO ARAC SCT (allo sibling or matched unrelated or auto SCT)* CNS 6MP/MTX SZ-Apherese No Donor Auto SCT* R CYCLO ARAC VM26 ARAC CYCLO ARAC VM26 ARAC HD-MTX ASP HD-MTX ASP MRD IR HR VHR IDA FLAG Donor Allo SCT* 6MP/MTX PEG-Asp 1000 500 PEG-Asp 2000 2000 i.th. MTX i.th. triple prophylaxis (HR/VHR) BM/MRD 1 48 52 104 4 8 12 16 20 24 28 32 36 40 44 58 66 74 82 90 98 weeks Prior Total dose: 4000 (6000) U/m² Now Total dose: 14000 (22000) U/m² GMALL Study Center (Gökbuget 12/2009)
GMALL Study 07/2003 – Asparaginase-Intensification SUMMARY • Increased PEG-ASP dose feasible 2. No increase of early mortality / toxicity 3. Promising interim results, despite short follow-up, for - molecular response - overall survival - remission duration 4. Major clinical problem in adult ALL: liver toxicity (no predictive factors beside age!) ASP is highly relevant for tx optimisation in adult ALL GMALL Study Center (Gökbuget 12/2009)
Survival After Transplant For ALL 100 Disease Free Survival (%) 80 FHCRC, Seattle 60 1st Remission (N = 41) 43% 40 2nd Remission (N = 46) 23% 20 P <0.001 0 0 2 4 6 8 10 12 YEARS Doney K et al, Biol Blood Marrow Transplant, 2003
Probability Of Survival After Allogeneic Transplants For All, Age >20 Years By Donor Type And Remission Status, 1994-1999 100 80 60 HLA-identical sibling, CR1 (N = 909) Probability, % 47% 40 25% HLA-identical sibling, CR2 (N = 388) 20 P = 0.0001 0 0 1 2 3 4 5 6 YEARS IBMTR data
MUD transplantation for adults with ALL (n=725) LFS BM 45 ± 3% PB 36 ± 3% P=0.03 years Basara et al. Blood 2007
treatment CR relapse 1012 clinical diagnosis diagnosis by morphology 1010 resistant disease MRD 108 106 Beyond detection limit 104 consolidation 102 cure
WHO 2008: “AML with recurrent genetic abnormalities”Provisional entities: AML with mutated NPM1 AML with mutated CEBPA Frequency, favorable prognostic significance in absence of FLT3-ITD, and association with certain morphologic and clinical features suggest they may identify unique subsets of AML Because of adverse prognostic impact of FLT3 mutations in AML with NPM1 mutations, mutational status of FLT3, NPM1 and CEBPA must all be performed in order to use these provisional entities
Prognostic significance of FLT3-ITD, CEBPA & NPM1 mutations as single markers in de novo adult CN-AML pts <60 yrs inCALGB 1.0 EFS at 5 yrs mut CEBPA 56% CEBPA 0.8 wt CEBPA 33% 1.0 0.6 mut CEBPA (n=36) FLT3-ITD negative FLT3-ITD 45% Event-Free Survival Low allelic ratio 25% 0.8 0.4 High allelic ratio 16% wt CEBPA (n=171) 0.6 0.2 ITD negative (n=158) FLT3 Event-Free Survival P =.02 0.4 0.0 Low allelic ratio (n=44) 1.0 0 1 2 3 4 5 6 7 8 9 10 11 NPM1 0.2 Years EFS at 5 yrs High allelic ratio (n=37) MutNPM1 41% 0.8 <.0001 P 0.0 wt NPM1 29% 0 1 2 3 4 5 6 7 8 9 10 11 0.6 Free Survival Years mut (n=138) NPM1 - 0.4 Event wt (n=76) NPM1 0.2 =.28 P 0.0 0 1 2 3 4 5 6 7 8 9 10 11 Years Whitman et al. Cancer Res 61:7233-9, 2001 Marcucci et al. JCO 26:5078-87, 2008 Paschka et al. Haematologica 92(suppl 1):145, 2007 CALGB 9621/19808 11/08 update
New Recommended Standardized Reporting for Correlation of Cytogenetic & Molecular Genetic Data with Clinical Data in AML* *International expert panel recommendations on behalf of the ELN (Döhner et al.)
Cytogenetic prognosis in de novo AML according tothe ELN recommendation (Döhner et al., 2005) N=287 curatively treated patients < 60 years (Olomouc and Plzeň data only) Cytogenetic prognosis: Very good (APL*) Intermediate 1 Intermediate 2 Good Poor Unachieved Age ML chi-square test:p = 0.034
Induction therapy of de novo AML (except APL) N=1183 (72.2%) Therapy: Curative Supportive only Palliative Age ML chi-square test:p < 0.001
Early deaths afterinduction treatment in de novo AML(except APL) N=854 (72.2%) Earlydeath (during 30 days from the diagnosis): Yes No Age ML chi-square test:p = 0.016
CR rate after induction therapy ofde novo AML (except APL) N=854 (72.2%) Therapeutic response: CR CR not achieved Age ML chi-square test:p < 0.001
Cytogenetic prognosis and achievement of CR in de novo AML (except APL) N=854 (72.2%) Therapeutic response: CR CR not achieved Age Cytogenetic prognosis: ML chi-square test:p = 0.010 Cytogenetic prognosis: ML chi-square test:p = 0.004 Cytogenetic prognosis: ML chi-square test:p < 0.001
Consolidationtherapy in de novo AMLpatients in CR(except APL) N=604 CR and consolidation CR, no consolidation Age ML chi-square test:p = 0.001
Type of consolidation in de novo AML (except APL) N=604 Consolidation: AutologousSCT AllogeneicSCT no consolidation Standard ID/HD Age ML chi-square test:p < 0.001
Time from diagnosis to SCT inde novo AML in the 1stCR(except APL) N=222 Time from diagnosis to transplantation(months) Transplantation N Mean Median Min-max Minimum Median Maximum