Download
1 / 29
310 likes | 549 Views
Prognostic Factors and Mechanisms of Resistance in mRCC:. Jorge A. Garcia, MD, FACP. Director, Advanced Prostate Cancer Program Cleveland Clinic Taussig Cancer Institute Glickman Urological & Kidney Institute Cleveland Clinic College of Medicine of CWRU. Madrid SOGUG, November 2010.

E N D
Prognostic Factors and Mechanisms of Resistance in mRCC: Jorge A. Garcia, MD, FACP. Director, Advanced Prostate Cancer Program Cleveland Clinic Taussig Cancer Institute Glickman Urological & Kidney Institute Cleveland Clinic College of Medicine of CWRU Madrid SOGUG, November 2010
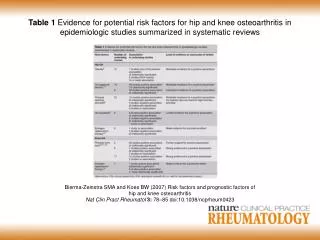
Prognostic Factors in RCC • What is their significance ? • Patient Counseling • Evaluation of clinical outcome • Identification poor-risk patients > Role of adjuvant Rx • Patient Selection for Clinical Trials • Interpreting results in clinical trials • Determinants of the Natural History of RCC • Tumor Related (TNM, Histology, Fuhrman Grade, # of Mets) • Patient Related (ECOG PS, Laboratory data) • Treatment Related Factors (Nephrectomy, therapy)
Prognostic Factors in RCC …Ideally, these should be molecular based factors. However, when results with molecular- based factors are disappointing, physicians often use clinical characteristics to make treatment decisions.
Metastatic RCC Prognosis: MSKCC Risk-Factor Model Greater number of risk factors is associated with worse prognosis* 100 0 risk factors (164 patients, 30 alive) 29.6m** 1 or 2 risk factors (348 patients, 23 alive) 10.3m** 80 3, 4, or 5 risk factors (144 patients, 1 alive) 4.9m** 60 Survival (%) *Risk factors: no prior nephrectomy, KPS <80, low HGB, high corrected calcium, high LDH. HGB=hemoglobin; KPS=Karnofsky performance status; LDH=lactate dehydrogenase. **Interval from Initial RCC Dx to IFN –a Therapy 40 20 0 13 0 1 2 3 4 5 6 7 8 9 10 11 12 14 15 16 17 Years following systemic therapy Adapted from Motzer RJ et al. J Clin Oncol. 1999;17:2530-2540.
Prognostic Factors in the VEGF Era Developed in first-line targeted therapy setting: • KPS<80 • Diagnosis to treatment interval < 1year • Anemia • Neutrophilia • Thrombocytosis • Hypercalcemia Tree Risk Groups • 0 factors: favorable prognosis • mOS 37 months • 1-2 factors: intermediate prognosis • mOS 27 months • 3+ factors: poor prognosis • mOS 8.8 months Heng DY et al. JCO 2009
Overall survival probability according to time after therapy initiation and risk group. Heng D Y et al. JCO 2009.
Clinical Prognostic Factors for Sunitinib Therapy: 12-Month PFS • Data from phase III trial of sunitinib vs IFN-α in frontline treatment of mRCC (N=375) • These factors have previously demonstrated prognostic value in models comprised of patients treated with cytokines or cytotoxics *Pretreatment factors that had the greatest influence on the nomogram’s predictions. Motzer. Cancer. 2008;113:1552.
Prognostic Factors Associated With OS in Patients Treated With Sunitinib • Analysis of prognostic factors for OS performed on data from a phase III trial of sunitinib vs IFN-α (N=750) • Selected pretreatment variables were evaluated using a Cox proportional hazards model *Prognostic factors previously identified in the MSKCC risk groups. ECOG=Eastern Cooperative Oncology Group; PS=performance status. Patil. ASCO. 2009 (abstr 5042).
TARGET: Prognostic Value of VEGF Low Baseline VEGF (≤131 pg/mL) High Baseline VEGF (>131 pg/mL) Median PFS Median PFS 5.5 mo P<0.01 HR=0.64 P<0.01 HR=0.48 5.5 mo 3.3 mo 2.7 mo PFS (%) PFS (%) Sorafenib (N=180) Sorafenib (N=184) Placebo (N=176) Placebo (N=172) Time Since Random Assignment (Months) Time Since Random Assignment (Months) • Analysis from phase III trial of sorafenib vs placebo in second-line treatment of mRCC • Both high and low baseline VEGF groups benefited from sorafenib • Patients with high VEGF levels, who are at an initial disadvantage with a poorer prognosis, might benefit more Adapted from Escudier. B, et al. J Clin Oncol. 2009.
VHL Status: Predictive of Response to VEGF-Targeted Therapy • 123 patients analyzed: clear-cell histology, prior nephrectomy (98%), good PS • Patients with a mutated or methylated VHL gene had an ORR of 41% compared with 31% in patients with wild-type VHL (P=0.34) • ORR to VEGF-targeted therapy 52% in patients with loss-of-function VHL mutations vs 31% in patients with wild-type VHL (P=0.04) • PFS and OS not significantly different based on VHL status Choueiri. J Urol. 2008;3:860.
Elevated Diastolic Blood Pressure May Predict Prolonged Survival With Axitinib OS • Patients with cytokine- or sorafenib-refractory mRCC treated with axitinib 1.0 0.8 0.6 0.4 0.2 0.0 Maximum dBP dBP ≥90 mm Hg (N=59) dBP <90 mm Hg (N=50) Survival Probability 0 50 100 150 Time (Weeks) dBP=diastolic blood pressure. Rixe. ASCO. 2009 (abstr 5045).
Hypertension May Predict Prolonged Survival With Sunitinib • Retrospective analysis of patients treated with first- or second-line sunitinib • ORR did not differ significantly between patients who were taking antihypertensive medication at baseline and those who were not HT=hypertension. Rini. KCA. 2009.
Clinical Outcome to Bevacizumab plus Interferon According to the Development of Grade 2 or Greater Hypertension (CALGB trial)* * Any relation to therapy according to CTC AE version 3.0 Harzstark et al. ASCO GU 2010
Prognostic and Predictive Factors for Targeted Therapies: Summary and Conclusion Prognostic models developed from experience with targeted agents identify factors similar to MSKCC Additional prognostic clinical factors identified/CCF MSKCC/CCF remains the standard for mRCC Prospective studies needed to identify utility of molecular biomarkers Incorporation of biomarkers in prognostic models will be necessary Understanding the influence of biomarkers on response/prognosis can aid in the design of new targeted therapies
Defining Resistant Disease • No standard definitions exist • Early laboratory data has not been validated • Clinically, there is heterogeneity in the way we practice • Drug failure • Host related • Physiologic resistance such as reduced absorbance, increased clearance, etc. indicating need for dose modification or drug holiday • Drug failure • Tumor related • Fundamental shift within the tumor microenvironment to alternative tumor-promoting pathway that would require a change in agents and maybe a change in target
RECIST vs. Progressive Disease Sorafenib treatment Abou-Alfa G, et al. EORTC-NCI-AACR 2004, Geneva, Switzerland
Change in tumor burden in mRCC patients Easy to call PD Easy to say NOT PD ???? PD Adapted from Elaraj et al. J Immunotx 27(4), 2004
Patterns of Tumor Progression vs. Selection of Subsequent Therapy Primary Refractory Early Progression Late Progression Change in TumorMeasurements (%) Change in TumorMeasurements (%) Change in TumorMeasurements (%)
Potential Mechanisms of RCC Treatment Resistance Rini BI and Atkins M. Lancet Oncol 2010.
Resistance Appears Mediated by “Angiogenic Escape” - ASL MRI: Rodent model Baseline Day 3 Day 9 Day 22 ASL MRI H & E CD34
A498 Model: Perfusion resumes in advance of tumor growth Courtesy of M. Atkins, Beth Israel
VEGF-TKIs Following Bevacizumab *Therapy assessed in study; ‡Whole cohortNR = not reported • Rini, et al. JCO 2008; 2. Drabkin, et al. ASCO 2007; 3. Garcia JA, et al. Cancer 2010 4. Rini, et al. ASCO GU 2008
Selected DataNovel Agents Following TKIs 1. Dudek, et al. Cancer 2009; 2. Rini BI, et al. JCO 2008; 3. DiLorenzo et al. JCO, 2009; 4. Garcia JA, et al. Cancer 2010; 5. Rini BI. JCO 2009; 6. MacKenzie MJ, et al. Annals Onc 2010; 7. Garcia JA, et al. ESMO 2009.
Ongoing Clinical Trials in mRCC:Sequential Therapies 1. NCT00678392; 2. NCT00474786; 3. NCT00732914; 4. NCT00903175
Summary Statements: Resistant Disease • Early resistance is related to “angiogenic escape” • Acquired resistance is often reversible • Tumor volume reduction should not be the only reason why RCC patients should discontinue therapy • Although Everolimus is the “standard of care” in the second-line setting; PFS/ORR data is not impressive, placebo (SOC?), other VEGF inhibitors have shown activity AND clinical trials should be the treatment of choice • Need to define the true mechanism of resistant disease at the molecular level; this would allow for a rational selection of any subsequent treatment