Download
1 / 58
580 likes | 623 Views
Learn how ultrasound imaging plays a crucial role in diagnosing and managing major salivary gland lesions. Discover the benefits of gray scale and Doppler techniques, including differentiation of benign and malignant nodules and assessing vascularity. Real cases with varied pathologies are explored.

E N D
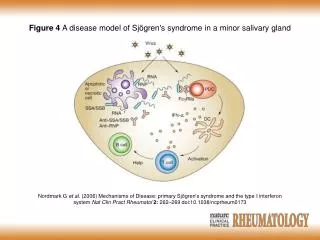
The Role of Gray Scale & Doppler Ultrasound in the Evaluation of Major Salivary Gland Lesions Dr.Rajeev.B.D Resident (III) SSGH & Medical college Vadodara 13/12/07
Role of Gray Scale & Doppler US • Ultrasound plays a significant and crucial role in the diagnosis and management of salivary gland lesions. • US is widely accepted as the first imaging method for assessment of major salivary glands. Results of the US examination alone may suggest the final diagnosis or provide important differential diagnostic data. • US can differentiate intraglandular from extraglandular lesions in 98% of cases. It can differentiate salivary gland lesions as focal or diffuse.
Further assessment of focal lesions and characterization of benignancy or malignancy can be done by evaluation of edges and adjacent adenopathy. With high resolution transducers ultrasound is better than CT scan or MRI in detection of unsharp borders. • Color Doppler sonography is a promising technique for analyzing the vascularity of the salivary glands and for characterizing pathologic conditions. • Color Doppler sonography help in differentiating pleomorphic adenomas from other salivary gland tumors.
A number of color Doppler criteria have been established to distinguish benign and malignant nodules. • US examination can be easily combined with fine needle aspiration cytology (FNAC), further enhancing its ability to differentiate between benign and malignant lesions. • Other benefits of US are easy availability, absent radiation, non-invasive & low cost.
Acute sialadenitis US & Doppler appearance • Salivary glands are enlarged and hypoechoic. • They may be inhomogeneous; may contain multiple small, oval, hypoechoic areas. • Increased blood flow.
Rana Subhadraben 35Y/F Rt pre-auricular region swelling&pain-5 Days
Chronic Sialadenitis US & Doppler appearance • Salivary glands are normal sized or smaller, hypoechoic, and inhomogeneous and • Mild or no increase in blood flow.
Rathod Durgaprasad 65Y/M Lt pre-auricular region pain-2 wks
Abscess • Abscesses are hypoechoic or anechoic lesions with posterior acoustic enhancement and unclear borders. • Central liquefaction may be distinguished as an avascular area or identified by means of moving debris. • Hyperechoic foci due to microbubbles of gas may be seen within the abscess.
Tarakesh Baburam 28Y/M Rt parotid region pain-20d Fever
Tuberculous parotitis • Parenchymal type of tuberculosis show focal, intraparotid, nearly anechoic zones that might have cavities within them. • In necrotic caseous cavities, no color flow signals can be detected at US, in contrast to most salivary tumors.
Vasava Reshmaben 6Y/F B/L neck & face swelling with fever-3m
Babubhai Ganeshbhai 52Y/M B/L parotid region pain-2m Non-specific lymphadenitis
Sialolithiasis US & Doppler appearance • For the detection of salivary calculi, ultrasound is the investigation of choice. • On ultrasound stones appear as hyperechoic foci casting posterior acoustic shadowing.
Pathan Siddikabanu 42Y/F Rt SMR pain-6m
Rathod Udesingh 52Y/M Rt SMR pain-4m
Benign lymphoepithelial lesion • Benign Lymphoepithelial Parotid Lesions in HIV-Positive patients are nodules that occur in the parotid gland as an early manifestation of HIV infection. • Wide spectrum of sonographic appearances, ranging from simple cysts to mixed masses with predominantly solid components.
50 Y/F HIV +ve B/L neck swelling – 3m
Pleomorphic adenoma US & Doppler appearance • Appears as a homogeneous, hypoechoic solid mass, usually less than 3cm in size. It is round or oval in shape and well-defined with lobulated margins with posterior acoustic enhancement. • Color Doppler sonography help in differentiating pleomorphic adenoma from other salivary gland tumors. Most pleomorphic adenoma show intermediate (1+ and 2+) grades of vascularity and a peripheral basketlike pattern. • When the pattern of tumor flow signals is peripheral, it could be considered specific enough to aid in diagnosing pleomorphic adenoma.
Vasava Ramilaben 35Y/F Lt parotid region swelling-1y
Pathan Memudaben 44Y/F Rt parotid region swelling-1yr
Vasava Ishwarbhai 35Y/M Lt parotid region swelling -3yr Large & heterogeneous
Macchi Ambubhai 50Y/M Lt parotid sweling-1Yr High PSV
Parmar Ashokbhai 45y/m Lt parotid region swelling-10yr Calcification
Warthin’s Tumor • At US, Warthin tumors are oval, hypoechoic, well-defined tumors and often contain multiple anechoic areas. • Show intermediate grade of vascularity and predominant hilar type of distribution.
Mali Kailashaben 45Y/F Rt parotid region-1yr
Oncocytoma • Similar to pleomorphic adenoma on ultrasound.
Lipoma • Appear as a well-defined, ovoid or elliptical, slightly hypoechoic mass that contains multiple echogenic lines parallel to the skin surface giving a typical striped or feathered appearance. • Shows a good compressibility . • Usually no flow signals are detected with color Doppler examination.
Pathan Ismailbhai 48Y/M Rt parotid-6m
Hemangioma • Typically they are heterogeneous hypoechoic lesions with sinusoidal spaces, internal slow flow and phleboliths on ultrasound.
Parmar Jignesh 1Y/M Rt parotid region swelling-6m
Giri Ramaben 45Y/F Rt parotid region swelling-1m
Fatty infiltration • Fatty infiltration causes diffuse, usually bilateral and homogeneous parotid enlargement. • Fatty infiltration can make ultrasound assessment of the parotid difficult due to beam attenuation obscuring deeper parts of the gland.
Patel Zarinaben 48Y/F B/L parotid swelling-1yr Rt parotid Lt parotid
Plunging ranula • US reveal smooth well delineated thin walled cystic lesion in the floor of mouth in case of simple ranula and extension of this lesion in submandibular space in case of plunging ranula.
Vasava Chaturbhai 35Y/M Rt SM region swelling-1m
Malignant tumors • US is the initial modality of choice. The ultrasound distinction of benign and malignant lesions is not precise, but certain features should raise suspicion for malignancy. • These include: if the margin of the lesion is ill-defined, locally invasive, if the mass is in the deep lobe, and if abnormal cervical lymph nodes are present. • Sonographically, the best indication of a malignant nodule is the absence of sharply defined margins.
Doppler criteria • Grade of intratumor vascularity-Grade 2/3 • Pattern of vascular supply-Mixed • Pulse-wave Doppler findings-PSV >25cm/sec, RI>0.8 and PI>1.8.
Parmar Motibhai 80y/m Lt parotid region swelling-15yr
Rathava Chitabhai 64y/m Rt parotid region swelling-5yr
Solanki Mahijibhai 60Y/M Rt parotid swelling-1yr Duadruparesis-1m